

Cone beam CT-based adaptive intensity modulated proton therapy assessment using automated planning for head-and-neck cancer
- PMID: 38263237
- PMCID: PMC10804468
- DOI: 10.1186/s13014-024-02406-9
Cone beam CT-based adaptive intensity modulated proton therapy assessment using automated planning for head-and-neck cancer
Abstract
Background: To assess the feasibility of CBCT-based adaptive intensity modulated proton therapy (IMPT) using automated planning for treatment of head and neck (HN) cancers.
Methods: Twenty HN cancer patients who received radiotherapy and had pretreatment CBCTs were included in this study. Initial IMPT plans were created using automated planning software for all patients. Synthetic CTs (sCT) were then created by deforming the planning CT (pCT) to the pretreatment CBCTs. To assess dose calculation accuracy on sCTs, repeat CTs (rCTs) were deformed to the pretreatment CBCT obtained on the same day to create deformed rCT (rCTdef), serving as gold standard. The dose recalculated on sCT and on rCTdef were compared by using Gamma analysis. The accuracy of DIR generated contours was also assessed. To explore the potential benefits of adaptive IMPT, two sets of plans were created for each patient, a non-adapted IMPT plan and an adapted IMPT plan calculated on weekly sCT images. The weekly doses for non-adaptive and adaptive IMPT plans were accumulated on the pCT, and the accumulated dosimetric parameters of two sets were compared.
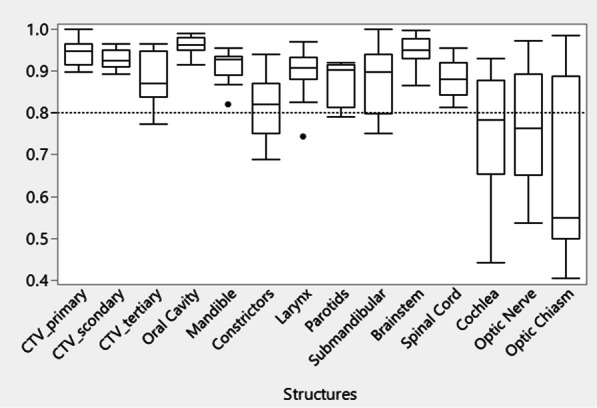
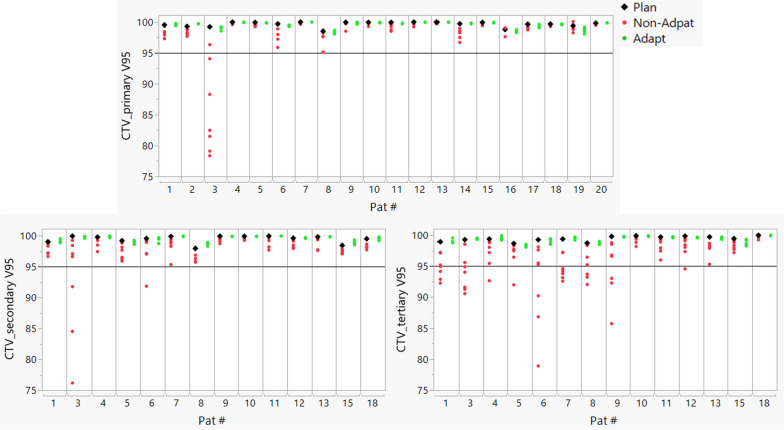
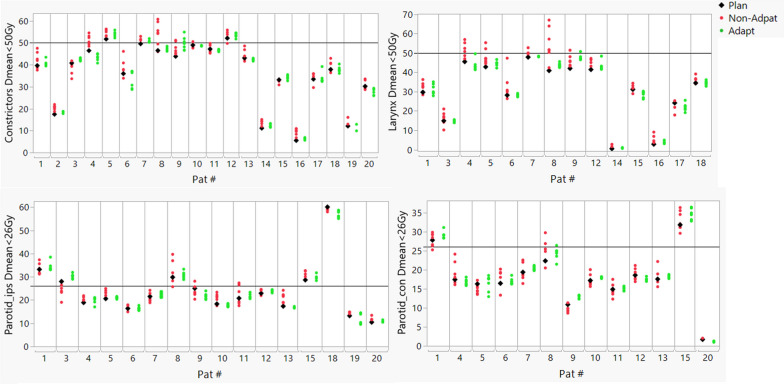
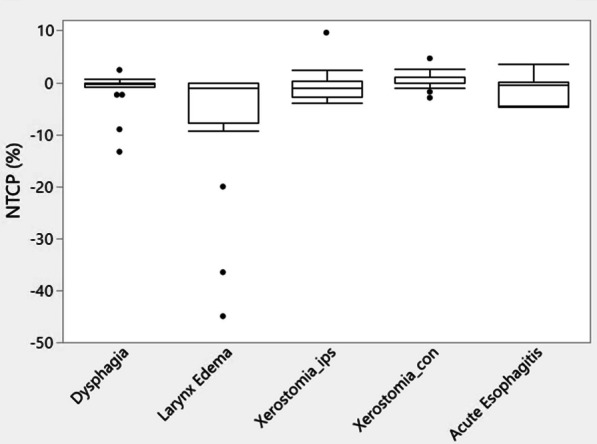
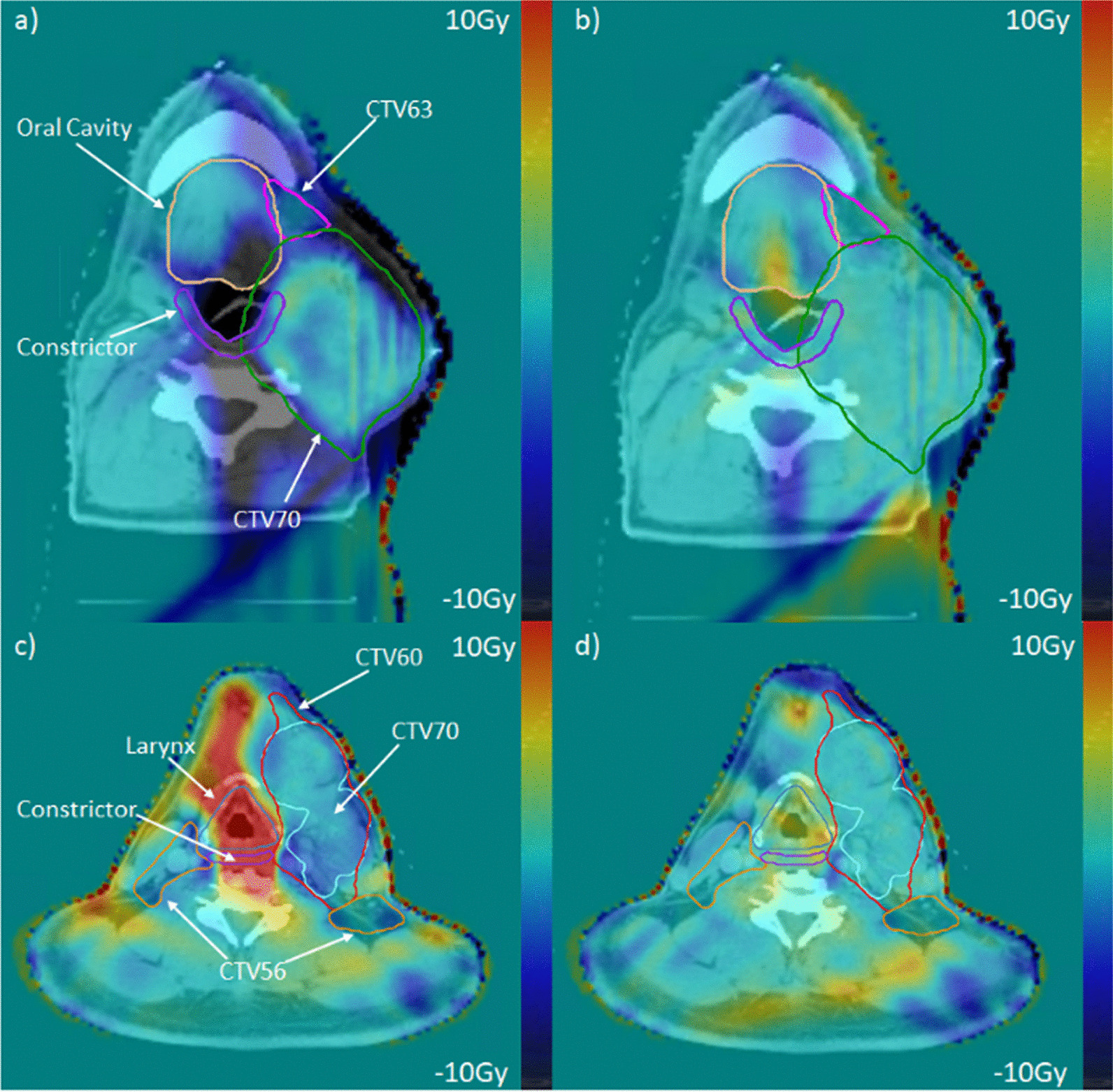
Results: Gamma analysis of the dose recalculated on sCT and rCTdef resulted in a passing rate of 97.9% ± 1.7% using 3 mm/3% criteria. With the physician-corrected contours on the sCT, the dose deviation range of using sCT to estimate mean dose for the most organ at risk (OARs) can be reduced to (- 2.37%, 2.19%) as compared to rCTdef, while for V95 of primary or secondary CTVs, the deviation can be controlled within (- 1.09%, 0.29%). Comparison of the accumulated doses from the adaptive planning against the non-adaptive plans reduced mean dose to constrictors (- 1.42 Gy ± 2.79 Gy) and larynx (- 2.58 Gy ± 3.09 Gy). The reductions result in statistically significant reductions in the normal tissue complication probability (NTCP) of larynx edema by 7.52% ± 13.59%. 4.5% of primary CTVs, 4.1% of secondary CTVs, and 26.8% tertiary CTVs didn't meet the V95 > 95% constraint on non-adapted IMPT plans. All adaptive plans were able to meet the coverage constraint.
Conclusion: sCTs can be a useful tool for accurate proton dose calculation. Adaptive IMPT resulted in better CTV coverage, OAR sparing and lower NTCP for some OARs as compared with non-adaptive IMPT.
Keywords: Adaptive; CBCT; Head and neck cancer; IMPT.
© 2024. The Author(s).
Conflict of interest statement
The authors declare there are no competing interests.
Figures



References
-
- Simone CB, II, Ly D, Dan TD, Ondos J, Ning H, Belard A, et al. Comparison of intensity-modulated radiotherapy, adaptive radiotherapy, proton radiotherapy, and adaptive proton radiotherapy for treatment of locally advanced head and neck cancer. Radiother Oncol. 2011;101(3):376–382. doi: 10.1016/j.radonc.2011.05.028. - DOI - PMC - PubMed
-
- van de Water TA, Lomax AJ, Bijl HP, de Jong ME, Schilstra C, Hug EB, et al. Potential benefits of scanned intensity-modulated proton therapy versus advanced photon therapy with regard to sparing of the salivary glands in oropharyngeal cancer. Int J Radiat Oncol Biol Phys. 2011;79(4):1216–1224. doi: 10.1016/j.ijrobp.2010.05.012. - DOI - PubMed
-
- Hague C, Aznar M, Dong L, Fotouhi-Ghiam A, Lee LW, Li T, et al. Inter-fraction robustness of intensity-modulated proton therapy in the post-operative treatment of oropharyngeal and oral cavity squamous cell carcinomas. Br J Radiol. 2020;93(1107):20190638. doi: 10.1259/bjr.20190638. - DOI - PMC - PubMed
-
- Langius JA, van Dijk AM, Doornaert P, Kruizenga HM, Langendijk JA, Leemans CR, et al. More than 10% weight loss in head and neck cancer patients during radiotherapy is independently associated with deterioration in quality of life. Nutr Cancer. 2013;65(1):76–83. doi: 10.1080/01635581.2013.741749. - DOI - PubMed
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
