

Cerebral autoregulation in traumatic brain injury: ultra-low-frequency pressure reactivity index and intracranial pressure across age groups
- PMID: 38263241
- PMCID: PMC10807228
- DOI: 10.1186/s13054-024-04814-5
Cerebral autoregulation in traumatic brain injury: ultra-low-frequency pressure reactivity index and intracranial pressure across age groups
Abstract
Background: The ultra-low-frequency pressure reactivity index (UL-PRx) has been established as a surrogate method for bedside estimation of cerebral autoregulation (CA). Although this index has been shown to be a predictor of outcome in adult and pediatric patients with traumatic brain injury (TBI), a comprehensive evaluation of low sampling rate data collection (0.0033 Hz averaged over 5 min) on cerebrovascular reactivity has never been performed.
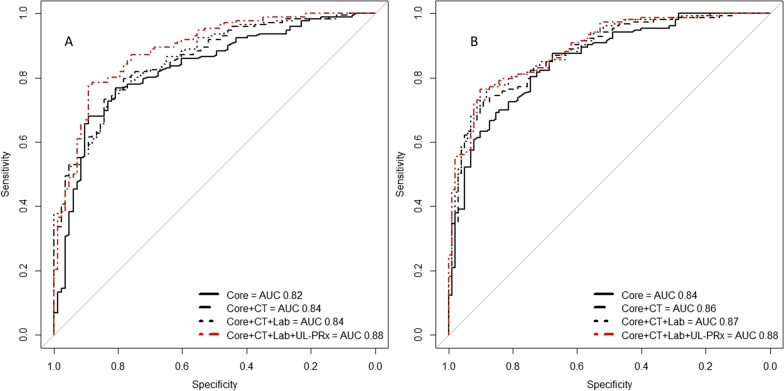
Objective: To evaluate the performance and predictive power of the UL-PRx for 12-month outcome measures, alongside all International Mission for Prognosis and Analysis of Clinical Trials (IMPACT) models and in different age groups. To investigate the potential for optimal cerebral perfusion pressure (CPPopt).
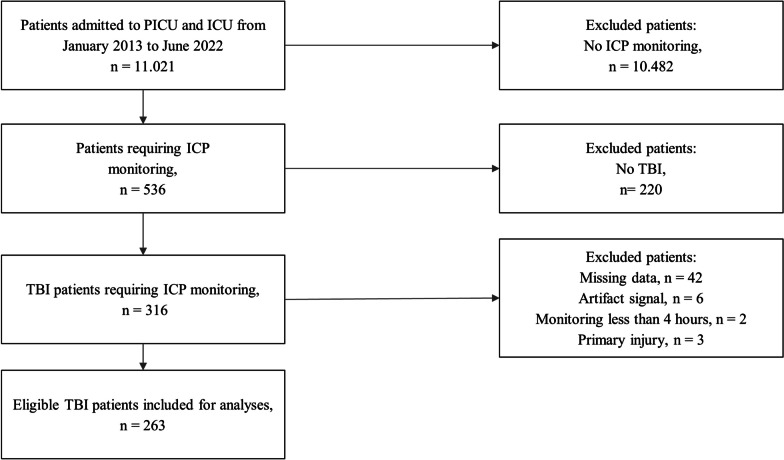
Methods: Demographic data, IMPACT variables, in-hospital mortality, and Glasgow Outcome Scale Extended (GOSE) at 12 months were extracted. Filtering and processing of the time series and creation of the indices (cerebral intracranial pressure (ICP), cerebral perfusion pressure (CPP), UL-PRx, and deltaCPPopt (ΔCPPopt and CPPopt-CPP)) were performed using an in-house algorithm. Physiological parameters were assessed as follows: mean index value, % time above threshold, and mean hourly dose above threshold.
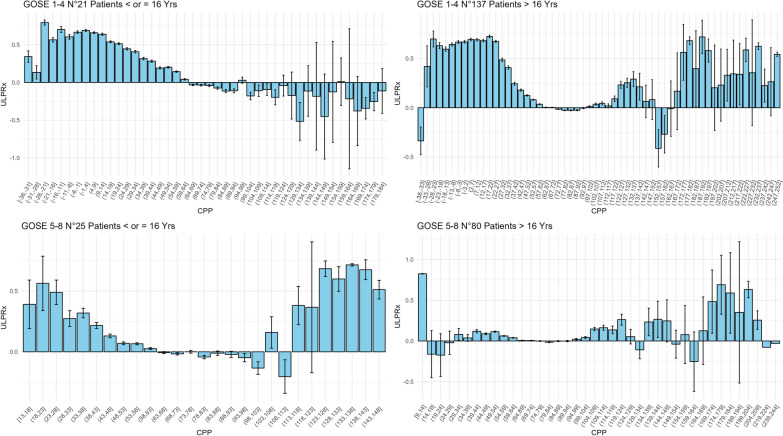
Results: A total of 263 TBI patients were included: pediatric (17.5% aged ≤ 16 y) and adult (60.5% aged > 16 and < 70 y and 22.0% ≥ 70 y, respectively) patients. In-hospital and 12-month mortality were 25.9% and 32.7%, respectively, and 60.0% of patients had an unfavorable outcome at 12 months (GOSE). On univariate analysis, ICP, CPP, UL-PRx, and ΔCPPopt were associated with 12-month outcomes. The cutoff of ~ 20-22 for mean ICP and of ~ 0.30 for mean UL-PRx were confirmed in all age groups, except in patients older than 70 years. Mean UL-PRx remained significantly associated with 12-month outcomes even after adjustment for IMPACT models. This association was confirmed in all age groups. UL-PRx resulted associate with CPPopt.
Conclusions: The study highlights UL-PRx as a tool for assessing CA and valuable outcome predictor for TBI patients. The results emphasize the potential clinical utility of the UL-PRx and its adaptability across different age groups, even after adjustment for IMPACT models. Furthermore, the correlation between UL-PRx and CPPopt suggests the potential for more targeted treatment strategies.
Trial registration: ClinicalTrials.gov identifier: NCT05043545, principal investigator Paolo Gritti, date of registration 2021.08.21.
Keywords: Age group; Cerebral autoregulation; Cerebrovascular reactivity; Intracranial pressure; Optimal cerebral perfusion pressure; Pressure reactivity index; Traumatic brain injury; Ultra-low-frequency pressure reactivity index.
© 2024. The Author(s).
Conflict of interest statement
The authors report no competing interests.
Figures

References
-
- Steiner LA, Czosnyka M, Piechnik SK, Smielewski P, Chatfield D, Menon DK, et al. Continuous monitoring of cerebrovascular pressure reactivity allows determination of optimal cerebral perfusion pressure in patients with traumatic brain injury. Crit Care Med. 2002;30:733–738. doi: 10.1097/00003246-200204000-00002. - DOI - PubMed
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
