

Symptoms and medical resource utilization of patients with bronchiectasis after SARS-CoV-2 infection
- PMID: 38264053
- PMCID: PMC10804846
- DOI: 10.3389/fmed.2023.1276763
Symptoms and medical resource utilization of patients with bronchiectasis after SARS-CoV-2 infection
Abstract
Background: The impact of COVID-19 caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) on patients with bronchiectasis in terms of symptoms, self-management and medical resource utilization was unknown.
Objective: To describe the impact of infection by SARS-CoV-2 on fluctuation of symptoms, self-management and medical resource utilization of patients with bronchiectasis during the pandemic of COVID-19.
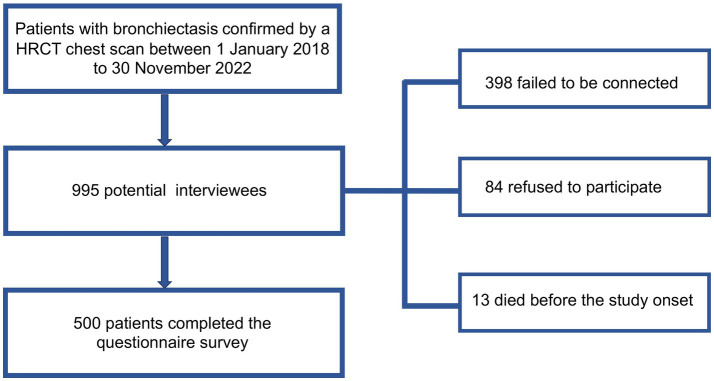
Methods: This was a single-center cross-sectional questionnaire study performed in Peking University Third Hospital. An online questionnaire investigation addressing the impact of SARS-CoV-2 infection on respiratory symptoms, self-management and medical resource utilization was conducted among patients with bronchiectasis during the COVID-19 surge in December 2022 in Beijing, China.
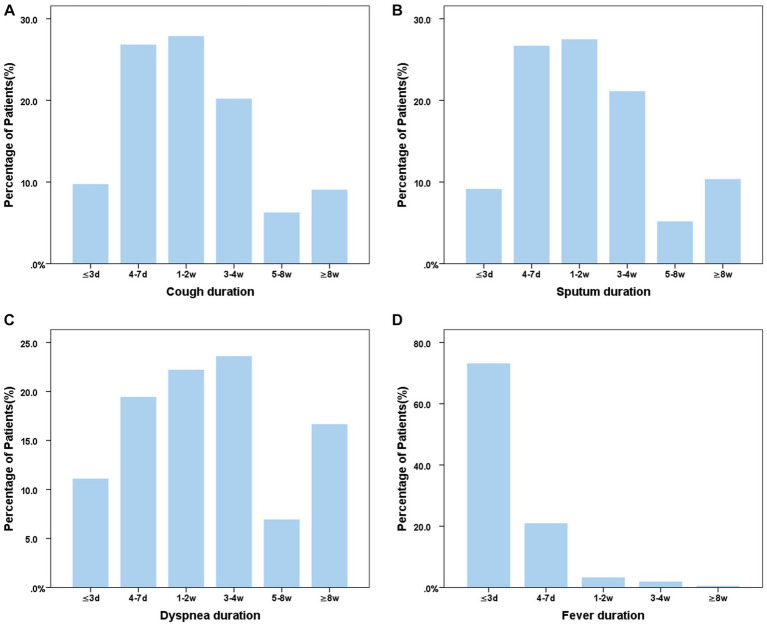
Results: Five hundred patients with bronchiectasis, with 285 (57%) females, and a mean () age of 57.9 15.1 years, completed the telephone questionnaire. The reported prevalence of COVID-19 was 81.2% (406/500). Of the 406 COVID-19 patients, 89.2% experienced fever lasting mostly for no more than 3 days, 70.6 and 61.8% reported exacerbated cough and sputum production respectively, and 17.7% reported worsened dyspnea. Notable 37.4% of the patients with COVID-19 experienced symptoms consistent with the definition of an acute exacerbation of bronchiectasis. However, 76.6% (311/406) of the infected patients did not seek medical care but managed at home. Of the patients who visited hospitals, 26.3% (25/95) needed hospitalization and 2.1% (2/95) needed ICU admission. Multi-factors logistic regression analysis showed that younger age (p = 0.012) and not using a bronchodilator agent(p = 0.022) were independently associated with SARS-CoV-2 infection, while a history of exacerbation of bronchiectasis in the past year (p = 0.006) and daily use of expectorants (p = 0.002) were associated with emergency visit and/or hospitalization for patients with bronchiectasis after SARS-CoV-2 infection.
Conclusion: During the COVID-19 surge, the infection rate of SARS-CoV-2 in patients with bronchiectasis was high, and most of the patients experienced new-onset or exacerbated respiratory symptoms, but only a minority needed medical visits. Our survey results further underscore the importance of patients' disease awareness and self-management skills during a pandemic like COVID-19.
Keywords: SARS-CoV-2; bronchiectasis; infection; medical resource; symptoms.
Copyright © 2024 Wang, Ren, Li, Wang, Chang, Sun and Sun.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Virtualized clinical studies to assess the natural history and impact of gut microbiome modulation in non-hospitalized patients with mild to moderate COVID-19 a randomized, open-label, prospective study with a parallel group study evaluating the physiologic effects of KB109 on gut microbiota structure and function: a structured summary of a study protocol for a randomized controlled study.Trials. 2021 Apr 2;22(1):245. doi: 10.1186/s13063-021-05157-0. Trials. 2021. PMID: 33810796 Free PMC article.
-
Self-Reported Symptoms of SARS-CoV-2 Infection in a Nonhospitalized Population in Italy: Cross-Sectional Study of the EPICOVID19 Web-Based Survey.JMIR Public Health Surveill. 2020 Sep 18;6(3):e21866. doi: 10.2196/21866. JMIR Public Health Surveill. 2020. PMID: 32650305 Free PMC article.
-
Post-COVID-19 Symptoms 2 Years After SARS-CoV-2 Infection Among Hospitalized vs Nonhospitalized Patients.JAMA Netw Open. 2022 Nov 1;5(11):e2242106. doi: 10.1001/jamanetworkopen.2022.42106. JAMA Netw Open. 2022. PMID: 36378309 Free PMC article.
-
Maternal and infant outcomes of full-term pregnancy combined with COVID-2019 in Wuhan, China: retrospective case series.Arch Gynecol Obstet. 2020 Sep;302(3):545-551. doi: 10.1007/s00404-020-05573-8. Epub 2020 Jul 21. Arch Gynecol Obstet. 2020. PMID: 32696241 Free PMC article. Review.
-
Signs and symptoms to determine if a patient presenting in primary care or hospital outpatient settings has COVID-19.Cochrane Database Syst Rev. 2021 Feb 23;2(2):CD013665. doi: 10.1002/14651858.CD013665.pub2. Cochrane Database Syst Rev. 2021. Update in: Cochrane Database Syst Rev. 2022 May 20;5:CD013665. doi: 10.1002/14651858.CD013665.pub3. PMID: 33620086 Free PMC article. Updated.
References
-
- Villamañán E, Sobrino C, Carpio C, Moreno M, Arancón A, Lara C, et al. . Inhaled bronchodilators use and clinical course of adult inpatients with Covid-19 pneumonia in Spain: a retrospective cohort study. Pulm Pharmacol Ther. (2021) 69:102007. doi: 10.1016/j.pupt.2021.102007, PMID: - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous