

Jaundice-predominant manifestation of Kawasaki disease in children
- PMID: 38264503
- PMCID: PMC10803413
- DOI: 10.3389/fped.2023.1281909
Jaundice-predominant manifestation of Kawasaki disease in children
Abstract
Background: A jaundice-predominant presentation of Kawasaki disease (KD) is atypical.
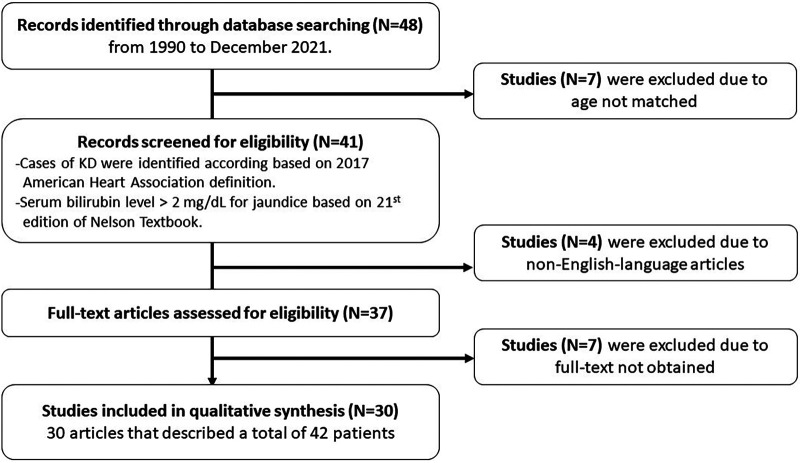
Methods: A total of 12 children with KD with a predominant manifestation of jaundice at MacKay Children's Hospital were reviewed, along with 42 cases reported in the literature since 1990.
Results: The median age of the 12 patients was 1.85 years (range: 3 months-4 years), and 66.6% were male. All of the patients had elevated liver function at presentation, 50% had hydrops of the gallbladder, and almost 60% had gastrointestinal symptoms and signs. Complete KD was evident in 11 of the 12 patients (91.7%), and two patients (16.7%) had recurrent episodes. All of the patients received intravenous immunoglobulin (IVIG); however, one-third were refractory to treatment. Corticosteroids were used in five (41.7%) of the patients. Three (25%) of the patients had shock, and seven (58.3%) had coronary artery abnormalities, of whom one (8.3%) had persistent coronary artery aneurysm and the others recovered. A review of the 42 cases in the literature showed that the children with a jaundice-predominant presentation of KD had high rates of IVIG-refractory disease (25%), coronary artery abnormalities (25%), shock (13.2%), and corticosteroid treatment (24.2%).
Conclusions: Children with KD presenting with a jaundice-predominant manifestation are at a higher risk of IVIG-refractory disease, coronary artery abnormalities, and more recurrent episodes. Physicians should be aware of the risk of shock in this population.
Keywords: IVIG-refractory disease; Kawasaki disease; children; hyperbilirubinemia; jaundice.
© 2024 Huang, Lin, Chi, Chiu, Huang, Chang, Kung and Huang.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Similar articles
-
Clinical features analysis of Kawasaki disease with abdominal symptoms as the first manifestation.Eur J Pediatr. 2023 Sep;182(9):4049-4057. doi: 10.1007/s00431-023-05086-x. Epub 2023 Jul 3. Eur J Pediatr. 2023. PMID: 37394531
-
Kawasaki disease at British Columbia's Children's Hospital.Paediatr Child Health. 2004 Sep;9(7):466-70. doi: 10.1093/pch/9.7.466. Paediatr Child Health. 2004. PMID: 19657410 Free PMC article.
-
Kawasaki disease shock syndrome: Unique and severe subtype of Kawasaki disease.Pediatr Int. 2018 Sep;60(9):781-790. doi: 10.1111/ped.13614. Pediatr Int. 2018. PMID: 29888440
-
Kawasaki disease: a comprehensive review of treatment options.J Clin Pharm Ther. 2015 Dec;40(6):620-5. doi: 10.1111/jcpt.12334. Epub 2015 Nov 7. J Clin Pharm Ther. 2015. PMID: 26547265 Review.
-
Hepatic predominant presentation of Kawasaki disease in adolescence case report and review of literature.BMC Gastroenterol. 2020 Oct 27;20(1):352. doi: 10.1186/s12876-020-01461-2. BMC Gastroenterol. 2020. PMID: 33109118 Free PMC article. Review.
Cited by
-
Unraveling the gut: the pivotal role of intestinal mechanisms in Kawasaki disease pathogenesis.Front Immunol. 2024 Nov 26;15:1496293. doi: 10.3389/fimmu.2024.1496293. eCollection 2024. Front Immunol. 2024. PMID: 39664384 Free PMC article. Review.
References
-
- Burns JC, Mason WH, Glode MP, Shulman ST, Melish ME, Meissner C, et al. Clinical and epidemiologic characteristics of patients referred for evaluation of possible Kawasaki disease. United States multicenter Kawasaki disease study group. J Pediatr. (1991) 118(5):680–6. 10.1016/S0022-3476(05)80026-5 - DOI - PubMed
-
- Falcini F, Resti M, Azzari C, Simonini G, Veltroni M, Lionetti P. Acute febrile cholestasis as an inaugural manifestation of Kawasaki’s disease. Clin Exp Rheumatol. (2000) 18(6):779–80. PMID: - PubMed
LinkOut - more resources
Full Text Sources