

Automatic triage of twelve-lead electrocardiograms using deep convolutional neural networks: a first implementation study
- PMID: 38264701
- PMCID: PMC10802816
- DOI: 10.1093/ehjdh/ztad070
Automatic triage of twelve-lead electrocardiograms using deep convolutional neural networks: a first implementation study
Abstract
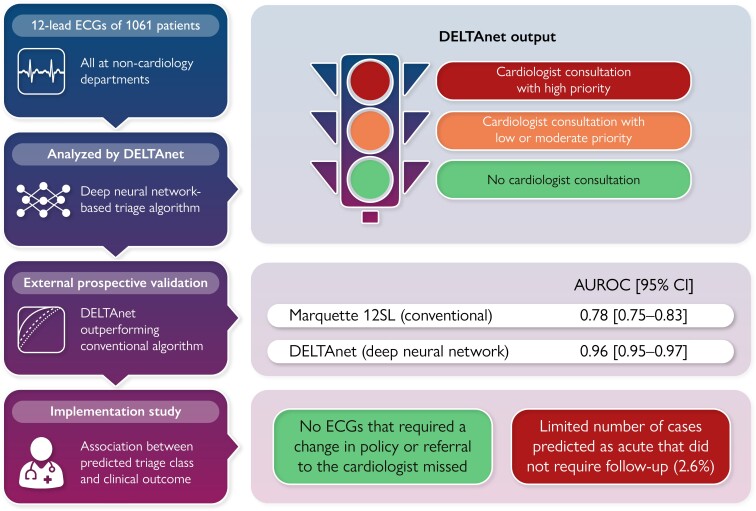
Aims: Expert knowledge to correctly interpret electrocardiograms (ECGs) is not always readily available. An artificial intelligence (AI)-based triage algorithm (DELTAnet), able to support physicians in ECG prioritization, could help reduce current logistic burden of overreading ECGs and improve time to treatment for acute and life-threatening disorders. However, the effect of clinical implementation of such AI algorithms is rarely investigated.
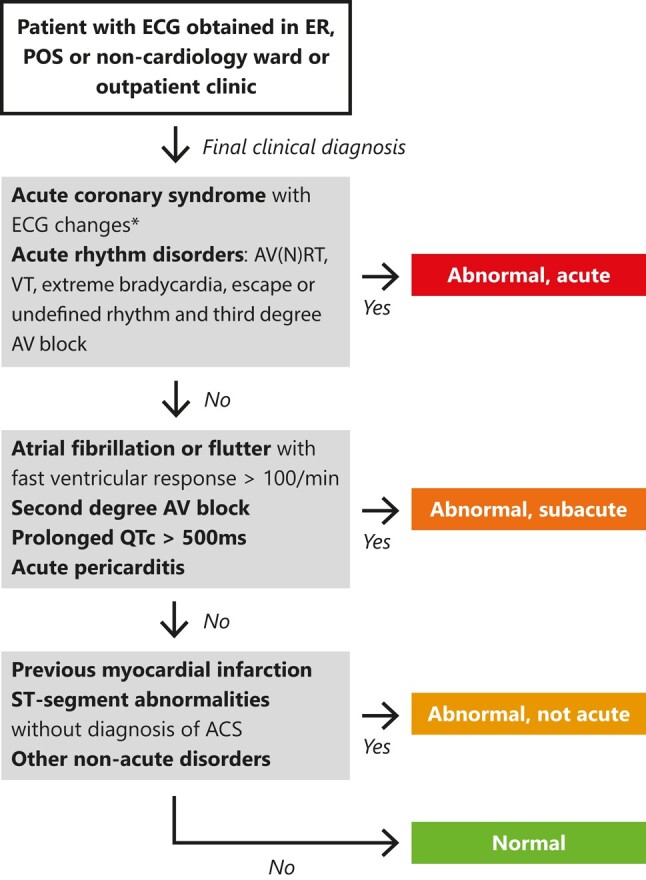
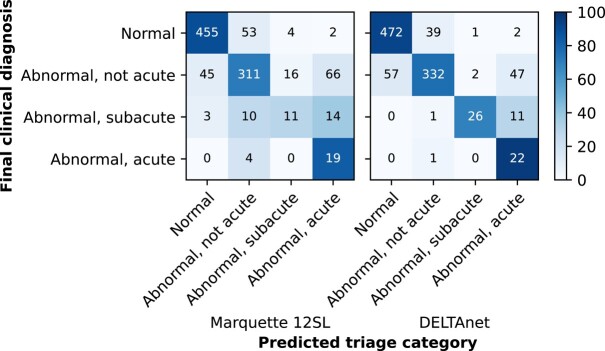
Methods and results: Adult patients at non-cardiology departments who underwent ECG testing as a part of routine clinical care were included in this prospective cohort study. DELTAnet was used to classify 12-lead ECGs into one of the following triage classes: normal, abnormal not acute, subacute, and acute. Performance was compared with triage classes based on the final clinical diagnosis. Moreover, the associations between predicted classes and clinical outcomes were investigated. A total of 1061 patients and ECGs were included. Performance was good with a mean concordance statistic of 0.96 (95% confidence interval 0.95-0.97) when comparing DELTAnet with the clinical triage classes. Moreover, zero ECGs that required a change in policy or referral to the cardiologist were missed and there was a limited number of cases predicted as acute that did not require follow-up (2.6%).
Conclusion: This study is the first to prospectively investigate the impact of clinical implementation of an ECG-based AI triage algorithm. It shows that DELTAnet is efficacious and safe to be used in clinical practice for triage of 12-lead ECGs in non-cardiology hospital departments.
Keywords: Deep learning; Electrocardiography; Implementation; Triage.
© The Author(s) 2023. Published by Oxford University Press on behalf of the European Society of Cardiology.
Conflict of interest statement
Conflict of interest: R.R.v.d.L. and R.v.E. are cofounders, shareholders, and board members of Cordys Analytics B.V., a spin-off of the UMC Utrecht that has licenced AI-ECG algorithms, including the algorithm studied in the current manuscript. The UMC Utrecht receives royalties from Cordys Analytics for potential future revenues. P.A.D. is a founder and shareholder of HeartEye B.V., an ECG device company.
Figures
Similar articles
-
Automatic Triage of 12-Lead ECGs Using Deep Convolutional Neural Networks.J Am Heart Assoc. 2020 May 18;9(10):e015138. doi: 10.1161/JAHA.119.015138. Epub 2020 May 14. J Am Heart Assoc. 2020. PMID: 32406296 Free PMC article.
-
Safety of Computer Interpretation of Normal Triage Electrocardiograms.Acad Emerg Med. 2017 Jan;24(1):120-124. doi: 10.1111/acem.13067. Acad Emerg Med. 2017. PMID: 27519772
-
Artificial intelligence-assisted remote detection of ST-elevation myocardial infarction using a mini-12-lead electrocardiogram device in prehospital ambulance care.Front Cardiovasc Med. 2022 Oct 14;9:1001982. doi: 10.3389/fcvm.2022.1001982. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 36312246 Free PMC article.
-
Artificial intelligence-enhanced electrocardiography for accurate diagnosis and management of cardiovascular diseases.J Electrocardiol. 2024 Mar-Apr;83:30-40. doi: 10.1016/j.jelectrocard.2024.01.006. Epub 2024 Jan 28. J Electrocardiol. 2024. PMID: 38301492 Review.
-
An Artificial Intelligence Analysis of Electrocardiograms for the Clinical Diagnosis of Cardiovascular Diseases: A Narrative Review.J Clin Med. 2024 Feb 11;13(4):1033. doi: 10.3390/jcm13041033. J Clin Med. 2024. PMID: 38398346 Free PMC article. Review.
Cited by
-
Deep learning for electrocardiogram interpretation: Bench to bedside.Eur J Clin Invest. 2025 Apr;55 Suppl 1(Suppl 1):e70002. doi: 10.1111/eci.70002. Eur J Clin Invest. 2025. PMID: 40191935 Free PMC article. Review.
-
Generative artificial intelligence for general practice; new potential ahead, but are we ready?Eur J Gen Pract. 2025 Dec;31(1):2511645. doi: 10.1080/13814788.2025.2511645. Epub 2025 Jun 6. Eur J Gen Pract. 2025. PMID: 40478782 Free PMC article.
-
Contrasting attitudes towards current and future artificial intelligence applications for computerised interpretation of electrocardiograms: a clinical stakeholder interview study.JAMIA Open. 2025 Jul 21;8(4):ooaf071. doi: 10.1093/jamiaopen/ooaf071. eCollection 2025 Aug. JAMIA Open. 2025. PMID: 40692805 Free PMC article.
-
Advancements in artificial intelligence-driven techniques for interventional cardiology.Cardiol J. 2024;31(2):321-341. doi: 10.5603/cj.98650. Epub 2024 Jan 22. Cardiol J. 2024. PMID: 38247435 Free PMC article. Review.
-
Towards prehospital risk stratification using deep learning for ECG interpretation in suspected acute coronary syndrome.BMJ Health Care Inform. 2025 Jun 6;32(1):e101292. doi: 10.1136/bmjhci-2024-101292. BMJ Health Care Inform. 2025. PMID: 40480678 Free PMC article.
References
-
- Ibanez B, James S, Agewall S, Antunes MJ, Bucciarelli-Ducci C, Bueno H, et al. 2017 ESC guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation. Eur Heart J 2018;39:119–177. - PubMed
-
- Foo CY, Bonsu KO, Nallamothu BK, Reid CM, Dhippayom T, Reidpath DD, et al. Coronary intervention door-to-balloon time and outcomes in ST-elevation myocardial infarction: a meta-analysis. Heart 2018;104:1362–1369. - PubMed
-
- Terkelsen CJ, Sørensen JT, Maeng M, Jensen LO, Tilsted H-H, Trautner S, et al. System delay and mortality among patients with STEMI treated with primary percutaneous coronary intervention. JAMA 2010;304:763–771. - PubMed
-
- Eslava D, Dhillon S, Berger J, Homel P, Bergmann S. Interpretation of electrocardiograms by first-year residents: the need for change. J Electrocardiol 2009;42:693–697. - PubMed
LinkOut - more resources
Full Text Sources