

Non-vitamin-K-antagonist oral anticoagulants (NOACs) after acute myocardial infarction: a network meta-analysis
- PMID: 38264795
- PMCID: PMC10806408
- DOI: 10.1002/14651858.CD014678.pub2
Non-vitamin-K-antagonist oral anticoagulants (NOACs) after acute myocardial infarction: a network meta-analysis
Abstract
Background: Balancing the risk of bleeding and thrombosis after acute myocardial infarction (AMI) is challenging, and the optimal antithrombotic therapy remains uncertain. The potential of non-vitamin K antagonist oral anticoagulants (NOACs) to prevent ischaemic cardiovascular events is promising, but the evidence remains limited.
Objectives: To evaluate the efficacy and safety of non-vitamin-K-antagonist oral anticoagulants (NOACs) in addition to background antiplatelet therapy, compared with placebo, antiplatelet therapy, or both, after acute myocardial infarction (AMI) in people without an indication for anticoagulation (i.e. atrial fibrillation or venous thromboembolism).
Search methods: We searched CENTRAL, MEDLINE, Embase, the Conference Proceedings Citation Index - Science, and two clinical trial registers in September 2022 with no language restrictions. We checked the reference lists of included studies for any additional trials.
Selection criteria: We searched for randomised controlled trials (RCTs) that evaluated NOACs plus antiplatelet therapy versus placebo, antiplatelet therapy, or both, in people without an indication for anticoagulation after an AMI.
Data collection and analysis: Two review authors independently checked the results of searches to identify relevant studies, assessed each included study, and extracted study data. We conducted random-effects pairwise analyses using Review Manager Web, and network meta-analysis using the R package 'netmeta'. We ranked competing treatments by P scores, which are derived from the P values of all pairwise comparisons and allow ranking of treatments on a continuous 0-to-1 scale.
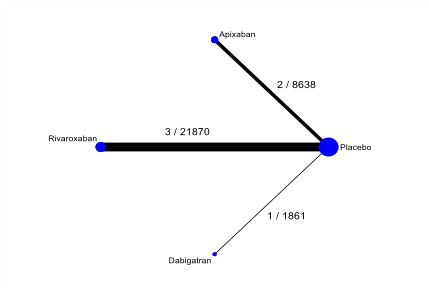
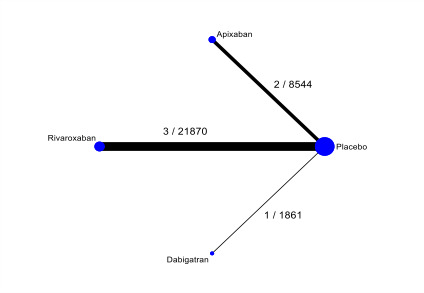
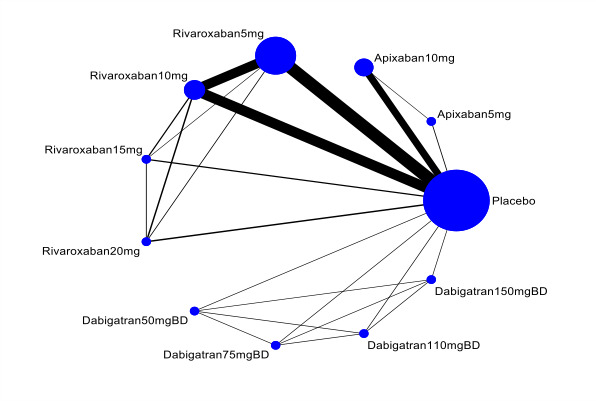
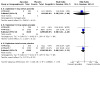
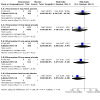
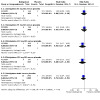
Main results: We identified seven eligible RCTs, including an ongoing trial that we could not include in the analysis. Of the six RCTs involving 33,039 participants, three RCTs compared rivaroxaban with placebo, two RCTs compared apixaban with placebo, and one RCT compared dabigatran with placebo. All participants in the six RCTs received concomitant antiplatelet therapy. The available evidence suggests that rivaroxaban compared with placebo reduces the rate of all-cause mortality (risk ratio (RR) 0.82, 95% confidence interval (CI) 0.69 to 0.98; number needed to treat for an additional beneficial outcome (NNTB) 250; 3 studies, 21,870 participants; high certainty) and probably reduces cardiovascular mortality (RR 0.83, 95% CI 0.69 to 1.01; NNTB 250; 3 studies, 21,870 participants; moderate certainty). There is probably little or no difference between apixaban and placebo in all-cause mortality (RR 1.09, 95% CI 0.88 to 1.35; number needed to treat for an additional harmful outcome (NNTH) 334; 2 studies, 8638 participants; moderate certainty) and cardiovascular mortality (RR 0.99, 95% CI 0.77 to 1.27; number needed to treat not applicable; 2 studies, 8638 participants; moderate certainty). Dabigatran may reduce the rate of all-cause mortality compared with placebo (RR 0.57, 95% CI 0.31 to 1.06; NNTB 63; 1 study, 1861 participants; low certainty). Dabigatran compared with placebo may have little or no effect on cardiovascular mortality, although the point estimate suggests benefit (RR 0.72, 95% CI 0.34 to 1.52; NNTB 143; 1 study, 1861 participants; low certainty). Two of the investigated NOACs were associated with an increased risk of major bleeding compared to placebo: apixaban (RR 2.41, 95% CI 1.44 to 4.06; NNTH 143; 2 studies, 8544 participants; high certainty) and rivaroxaban (RR 3.31, 95% CI 1.12 to 9.77; NNTH 125; 3 studies, 21,870 participants; high certainty). There may be little or no difference between dabigatran and placebo in the risk of major bleeding (RR 1.74, 95% CI 0.22 to 14.12; NNTH 500; 1 study, 1861 participants; low certainty). The results of the network meta-analysis were inconclusive between the different NOACs at all individual doses for all primary outcomes. However, low-certainty evidence suggests that apixaban (combined dose) may be less effective than rivaroxaban and dabigatran for preventing all-cause mortality after AMI in people without an indication for anticoagulation.
Authors' conclusions: Compared with placebo, rivaroxaban reduces all-cause mortality and probably reduces cardiovascular mortality after AMI in people without an indication for anticoagulation. Dabigatran may reduce the rate of all-cause mortality and may have little or no effect on cardiovascular mortality. There is probably no meaningful difference in the rate of all-cause mortality and cardiovascular mortality between apixaban and placebo. Moreover, we found no meaningful benefit in efficacy outcomes for specific therapy doses of any investigated NOACs following AMI in people without an indication for anticoagulation. Evidence from the included studies suggests that rivaroxaban and apixaban increase the risk of major bleeding compared with placebo. There may be little or no difference between dabigatran and placebo in the risk of major bleeding. Network meta-analysis did not show any superiority of one NOAC over another for our prespecified primary outcomes. Although the evidence suggests that NOACs reduce mortality, the effect size or impact is small; moreover, NOACs may increase major bleeding. Head-to-head trials, comparing NOACs against each other, are required to provide more solid evidence.
Copyright © 2024 The Authors. Cochrane Database of Systematic Reviews published by John Wiley & Sons, Ltd. on behalf of The Cochrane Collaboration.
Conflict of interest statement
SAS: no conflicts of interest. KK: no conflicts of interest. WS: no conflicts of interest; works as an interventional cardiologist in Halifax. DA: no conflicts of interest. DD: speaker honoraria from Bayer Healthcare, Pfizer Canada Inc., Daiichi Sankyo; published opinions for Deutsche Medizinische Wochenschrift; works as a health professional at University Medical Center Mannheim, Germany. RFS: consultant for Alnylam Pharmaceuticals, AstraZeneca, Bayer, Bristol Myers Squibb, Chiesi Farmaceutici, CSL Behring, Cytosorbents, GlyCardial Diagnostics, Hengrui, Idorsia, Intas Pharmaceuticals, Pfizer UK, Novartis, PhaseBio, Sanofi Aventis, Thromboserin; works as a health professional at Sheffield Teaching Hospitals NHS Foundation Trust. CMG: consultant for AstraZeneca, Bayer HealthCare Pharmaceuticals Inc., CSL Behring, Janssen Global Services, LLC, Johnson & Johnson Health Care Systems Inc.; Physician at Beth Israel Deaconess Medical Center. DW: consultant for Bayer, AstraZeneca, ABIOMED, Novartis. SA: no conflicts of interest; Cardiac Radiologist at Sheffield Teaching Hospitals.
Figures





































































































Update of
- doi: 10.1002/14651858.CD014678
References
References to studies included in this review
APPRAISE 1 {published data only}
-
- APPRAISE Steering Committee and Investigators, Alexander JH, Becker RC, Bhatt DL, Cools F, Crea F, et al. Apixaban, an oral, direct, selective factor Xa inhibitor, in combination with antiplatelet therapy after acute coronary syndrome: results of the Apixaban for Prevention of Acute Ischemic and Safety Events (APPRAISE) trial. Circulation 2009;119(22):2877-85. - PubMed
-
- NCT00313300. Safety study of apixaban in recent acute coronary syndrome [A phase 2, placebo-controlled, randomized, double blind, parallel arm, dose ranging study to evaluate safety and efficacy of apixaban in patients with a recent acute coronary syndrome]. clinicaltrials.gov/show/NCT00313300 (first received 12 April 2006).
APPRAISE 2 {published data only}
-
- Alexander JH, Lopes RD, James S, Kilaru R, He Y, Mohan P, et al. Apixaban with antiplatelet therapy after acute coronary syndrome. New England Journal of Medicine 2011;365(8):699-708. - PubMed
-
- Cornel J, James S, Wallentin L, Lopes RD, Neely M, Alexander JH, et al. Apixaban after acute coronary syndrome in patients with heart failure: insights from the APPRAISE-2 trial. European Heart Journal 2012;33(Suppl 1):335-6.
-
- Cornel JH, Lopes RD, James S, Stevens SR, Neely ML, Liaw D, et al. Anticoagulant therapy and outcomes in patients with prior or acute heart failure and acute coronary syndromes: insights from the APixaban for PRevention of Acute ISchemic Events 2 trial. American Heart Journal 2015;169(4):531-8. - PubMed
-
- Hagstrom E, Wallentin L, Wojdyla D, Neely ML, Stevens SR, Alexander JH, et al. Management and clinical consequences of major bleeding in high-risk patients following an acute coronary syndrome. Is aspirin the problem? Insights from the APPRAISE-2 trial. European Heart Journal 2015;36 Suppl 1:861-2.
ATLAS ACS {published data only}
-
- AlKhalfan F, Kerneis M, Nafee T, Yee Megan K, Chi G, Plotnikov A, et al. D-Dimer levels and effect of rivaroxaban on those levels and outcomes in patients with acute coronary syndrome (An ATLAS ACS-TIMI 46 Trial Substudy). American Journal of Cardiology 2018;122(9):1459-64. - PubMed
-
- Alkhalfan F, Kerneis M, Nafee T, Yee Megan K, Chi G, Plotnikov A, et al. D-dimer levels and clinical outcomes in acute coronary syndrome patients: an ATLAS ACS TIMI 46 trial substudy. Circulation 2018;138. - PubMed
-
- Geller BJ, Mega JL, Morrow DA, Guo J, Hoffman EB, Gibson MC, et al. Autoantibodies to phosphorylcholine and cardiovascular outcomes in patients with acute coronary syndromes in the ATLAS ACS-TIMI 46 trial. Journal of Thrombosis and Thrombolysis 2014;37(3):310-6. - PubMed
-
- Mega JL, Braunwald E, Mohanavelu S, Burton P, Poulter R, Misselwitz F, et al. Rivaroxaban versus placebo in patients with acute coronary syndromes (ATLAS ACS-TIMI 46): a randomised, double-blind, phase II trial. Lancet 2009;374(9683):29-38. - PubMed
-
- NCT00402597. Rivaroxaban in combination with aspirin alone or with aspirin and a thienopyridine in patients with acute coronary syndromes (The ATLAS ACS TIMI 46 Trial) [A randomized, double-blind, placebo-controlled, multicenter, dose-escalation and dose-confirmation study to evaluate the safety and efficacy of rivaroxaban in combination with aspirin alone or with aspirin and a thienopyridine in subjects with acute coronary syndromes]. clinicaltrials.gov/show/NCT00402597 (first received 22 November 2006).
ATLAS ACS 2 {published data only}
-
- Alkhalfan F, Nafee T, Yee M, Chi GC, Kalayci A, Plotnikov A, et al. The association of white blood cell count and bleeding in acute coronary syndrome: an insight into the ATLAS ACS-TIMI 51 trial. Circulation 2019;140 Suppl 1.
-
- Alkhalfan F, Nafee T, Yee MK, Chi G, Kalayci A, Plotnikov A, et al. Relation of white blood cell count to bleeding and ischemic events in patients with acute coronary syndrome (from the ATLAS ACS 2-TIMI 51 Trial). American Journal of Cardiology 2020;125(5):661-9. - PubMed
-
- Arora R, Lang C, Quddus A. Bayesian net-clinical benefit analysis of rivaroxaban in patients with acute coronary syndromes. Journal of the American College of Cardiology 2013;61(10 Suppl 1):E1534.
-
- Cavender M, Braunwald E, Gibson CM, Wiviott S, Murphy S, Amuchastegui M, et al. Rivaroxaban reduces spontaneous and large myocardial infarctions: findings from the ATLAS ACS 2 – TIMI 51 trial. Journal of the American College of Cardiology 2013;61(10 Suppl 1):E3.
-
- Cavender MA, Gibson CM, Braunwald E, Wiviott SD, Murphy SA, Toda KE, et al. The effect of rivaroxaban on myocardial infarction in the ATLAS ACS 2 – TIMI 51 trial. European Heart Journal 2015;4(5):468-74. - PubMed
GEMINI‐ACS {published data only}
-
- NCT02293395. A study to compare the safety of rivaroxaban versus acetylsalicylic acid in addition to either clopidogrel or ticagrelor therapy in participants with acute coronary syndrome [A randomized, double-blind, double-dummy, active-controlled, parallel-group, multicenter study to compare the safety of rivaroxaban versus acetylsalicylic acid in addition to either clopidogrel or ticagrelor therapy in subjects with acute coronary syndrome]. clinicaltrials.gov/show/NCT02293395 (first received 18 November 2014).
-
- Ohman EM, Roe MT, Steg PG, James SK, Povsic TJ, White J, et al. Clinically significant bleeding with low-dose rivaroxaban versus aspirin, in addition to P2Y12 inhibition, in acute coronary syndromes (GEMINI-ACS-1): a double-blind, multicentre, randomised trial. Lancet 2017;389(10081):1799-808. - PubMed
-
- Povsic TJ, Roe MT, Ohman EM, Steg PG, James S, Plotnikov A, et al. A randomized trial to compare the safety of rivaroxaban vs aspirin in addition to either clopidogrel or ticagrelor in acute coronary syndrome: the design of the GEMINI-ACS-1 phase II study. American Heart Journal 2016;174:120-8. - PubMed
REDEEM {published data only}
-
- NCT00621855. RE-DEEM dose finding study for dabigatran etexilate in patients with acute coronary syndrome [Randomised dabigatran etexilate dose finding study in patients with acute coronary syndromes post index event with additional risk factors for cardiovascular complications also receiving aspirin and clopidogrel: multi-centre, prospective, placebo controlled, group dose escalation trial (RE-DEEM study)]. clinicaltrials.gov/show/NCT00621855 (first received 22 February 2008).
-
- Oldgren J, Budaj A, Granger CB, Khder Y, Roberts J, Siegbahn A, et al. Dabigatran vs. placebo in patients with acute coronary syndromes on dual antiplatelet therapy: a randomized, double-blind, phase II trial. European Heart Journal 2011;32(22):2781-9. - PubMed
-
- Oldgren J, Wallentin L, Budaj A, Granger CB, Harper R, Khder Y, et al. Randomised dabigatran etexilate dose finding study in patients with acute coronary syndromes post index event with additional risk factors for cardiovascular complications also receiving aspirin and clopidogrel (RE-DEEM). Circulation 2010;120(21):2160-1.
References to studies excluded from this review
Alizadeh 2019 {published data only}
-
- Alizadeh M, Antoniou S, Fhadil S, Rathod R, Guttmann O, Knight C, et al. The use of direct oral anti-coagulations (DOACs) compared to vitamin K antagonist in patients with left ventricular thrombus after acute myocardial infarction. European Heart Journal 2019;40(Suppl 1):4026.
Borst 2018 {published data only}
Devereaux 2018 {published data only}
-
- Devereaux PJ, Duceppe E, Guyatt G, Tandon V, Rodseth R, Biccard BM, et al. Dabigatran in patients with myocardial injury after non-cardiac surgery (MANAGE): an international, randomised, placebo-controlled trial. Lancet 2018;391(10137):2325-34. - PubMed
Duceppe 2018 {published data only}
-
- Duceppe E, Yusuf S, Tandon V, Rodseth R, Biccard BM, Xavier D, et al. Design of a randomized placebo-controlled trial to assess dabigatran and omeprazole in patients with myocardial injury after noncardiac surgery (MANAGE). Canadian Journal of Cardiology 2018;34(3):295-302. - PubMed
Euctr 2013a {published data only}
-
- EUCTR2012-004180-43-CZ. Rivaroxaban for the prevention of major cardiovascular events in coronary or peripheral artery disease. www.who.int/trialsearch/Trial2.aspx?TrialID=EUCTR2012-004180-43-CZ 2013.
Euctr 2013b {published data only}
-
- EUCTR2013-000046-19-BG. A study to assess the effectiveness and safety of rivaroxaban in reducing the risk of death, myocardial infarction or stroke in participants with heart failure and coronary artery disease following an episode of decompensated heart failure. www.who.int/trialsearch/Trial2.aspx?TrialID=EUCTR2013-000046-19-BG 2013.
Gao 2015 {published data only}
-
- Gao F, Shen H, Wang Z, Yang S, Liu X, Zhou Y. Risk of hemorrhagic and ischemic stroke for dual antiplatelet therapy and new generation oral anticoagulants in patients with acute coronary syndrome. Journal of the American College of Cardiology 2015;66(16 Suppl 1):C158.
Greenberg 2018a {published data only}
-
- Greenberg BH, Anker SD, Byra WM, Nessel CC, Cleland JG, Fu M, et al. Effects of rivaroxaban on thrombotic events in heart failure patients with coronary disease and sinus rhythm. Circulation 2018;138(25):e761-2.
Greenberg 2018b {published data only}
-
- Greenberg B, Anker S, Byra WM, Fu M, Nessel CC, Cleland JG, et al. A randomized study comparing rivaroxaban with placebo in subjects with heart failure and significant coronary artery disease following an episode of decompensated heart failure: the COMMANDER HF study. Journal of Cardiac Failure 2018;24(11):811.
Kopin 2016 {published data only}
-
- Kopin D, Sherwood MW, Jones WS, Granger CB, Lopes RD, Alexander JH, et al. Percutaneous coronary intervention and antiplatelet therapy on apixaban or warfarin: insights from the ARISTOTLE trial. Circulation 2016;134:Suppl 1.
Lee 2018 {published data only}
-
- Lee J, Nakanishi R, Li D, Shaikh K, Shekar C, Osawa K, et al. Randomized trial of rivaroxaban versus warfarin in the evaluation of progression of coronary atherosclerosis. American Heart Journal 2018;206:127-30. - PubMed
NCT04333407 {published data only}
-
- NCT04333407. Preventing cardiac complication of COVID-19 disease with early acute coronary syndrome therapy: a randomised controlled trial. clinicaltrials.gov/show/NCT04333407 (first received 3 April 2020).
NCT04688723 {published data only}
-
- NCT04688723. Dual therapy with dabigatran/ticagrelor versus dual therapy with dabigatran/clopidogrel in ACS patients with indication for NOAC undergoing PCI. clinicaltrials.gov/show/NCT04688723 (first received 30 December 2020).
NCT04805710 {published data only}
-
- NCT04805710. Rivaroxaban or aspirin in patients with CHD & GD undergoing PCI. clinicaltrials.gov/show/NCT04805710 (first received 18 March 2021).
NCT04838808 {published data only}
-
- NCT04838808. Rivaroxaban in type 2 myocardial infarctions. clinicaltrials.gov/show/NCT04838808 (first received 9 April 2021).
Nct 2012 {published data only}
-
- NCT01661101. Management of myocardial injury after noncardiac surgery trial. clinicaltrials.gov/show/NCT01661101 (first received 9 August 2012).
Schiele 2018 {published data only}
-
- Schiele F, Puymirat E, Ferrieres J, Simon T, Danchin N. Do randomized clinical trial selection criteria reflect real-life levels of risk in acute myocardial infarction survivors? the compass trial in light of the FAST-MI 2005-2010-2015 registries. Circulation 2018;138:Suppl 1.
Zannad 2015 {published data only}
-
- Zannad F, Greenberg B, Cleland JG, Gheorghiade M, Veldhuisen DJ, Mehra MR, et al. Rationale and design of a randomized, double-blind, event-driven, multicentre study comparing the efficacy and safety of oral rivaroxaban with placebo for reducing the risk of death, myocardial infarction or stroke in subjects with heart failure and significant coronary artery disease following an exacerbation of heart failure: the COMMANDER HF trial. European Journal of Heart Failure 2015;17(7):735-42. - PMC - PubMed
Zannad 2018 {published data only}
-
- Zannad F, Anker SD, Byra WM, Cleland JG, Fu M, Gheorghiade M, et al. Rivaroxaban in patients with heart failure, sinus rhythm, and coronary disease. New England Journal of Medicine 2018;379(14):1332-42. - PubMed
References to ongoing studies
NCT03775746 {published data only}
-
- NCT03775746. Can very low dose rivaroxaban in addition to dual antiplatelet therapy (DAPT) improve thrombotic status in acute coronary syndrome (ACS) ACS (VaLiDate-R). clinicaltrials.gov/show/NCT03775746 (first received 14 December 2018).
Additional references
Al Said 2018
-
- Al Said S, Bode C, Duerschmied D. Anticoagulation in Atherosclerotic Disease. Hamostaseologie 2018;38(4):240-6. - PubMed
Al Said 2021
-
- Al Said S, Alabed S, Sumaya W, Alsaid D, Kaier K, Duerschmied D, et al. Non-vitamin-K-antagonist oral anticoagulants (NOACs) after acute myocardial infarction: a network meta-analysis. Cochrane Database of Systematic Reviews 2021, Issue 5. Art. No: CD014678. [DOI: 10.1002/14651858.CD014678] - DOI - PMC - PubMed
Alexander 2009
-
- Alexander JH, Becker RC, Bhatt DL, Cools F, Crea F, Dellborg M, et al. Apixaban, an oral, direct, selective factor Xa inhibitor, in combination with antiplatelet therapy after acute coronary syndrome: results of the Apixaban for Prevention of Acute Ischemic and Safety Events (APPRAISE) trial. Circulation 2009;119(22):2877-85. - PubMed
Alexander 2011
-
- Alexander JH, Lopes RD, James S, Kilaru R, He Y, Mohan P, et al. Apixaban with antiplatelet therapy after acute coronary syndrome. New England Journal of Medicine 2011;365(8):699-708. - PubMed
Amsterdam 2014
-
- Amsterdam EA, Wenger NK, Brindis RG, Casey DE, Ganiats TG, Holmes DR, et al. 2014 AHA/ACC guideline for the management of patients with non-ST-elevation acute coronary syndromes: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Journal of the American College of Cardiology 2014;64(24):e139-e228. - PubMed
Anand 2003
-
- Anand SS, Yusuf S. Oral anticoagulants in patients with coronary artery disease. Journal of the American College of Cardiology 2003;41:62S-69S. - PubMed
Andreotti 2006
-
- Andreotti F, Testa L, Biondi-Zoccai GG, Crea F. Aspirin plus warfarin compared to aspirin alone after acute coronary syndromes: an updated and comprehensive meta-analysis of 25,307 patients. European Heart Journal 2006;27:519-26. - PubMed
Bauer 2013
-
- Bauer KA. Pros and cons of new oral anticoagulants. Hematology 2013;2013:464-70. - PubMed
Bonaca 2015
-
- Bonaca MP, Bhatt DL, Cohen M, Steg PG, Storey RF, Jensen EC, et al. Long-term use of ticagrelor in patients with prior myocardial infarction. New England Journal of Medicine 2015;372(19):1791-800. - PubMed
Brignardello‐Petersen 2020
Chaimani 2022
-
- Chaimani A, Caldwell DM, Li T, Higgins JP, Salanti G. Chapter 11: Undertaking network meta-analyses. In: Higgins JP, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, Welch VA, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 6.3 (updated February 2022). Cochrane, 2022. Available from training.cochrane.org/handbook/archive/v.6.3.
Chesebro 1987
-
- Chesebro JH, Knatterud G, Roberts R, Borer J, Cohen LS, Dalen J, et al. Thrombolysis in Myocardial Infarction (TIMI) Trial, Phase I: a comparison between intravenous tissue plasminogen activator and intravenous streptokinase. Clinical findings through hospital discharge. Circulation 1987;76(1):142-54. - PubMed
Chiarito 2018
Cohen 1998
-
- Cohen J. Statistical Power Analysis for the Behavioral Sciences. 2nd edition. Hillsdale (NJ): L. Erlbaum Associates, 1998.
Collet 2020
-
- Collet J-P, Thiele H, Barbato E, Barthélémy O, Bauersachs J, Bhatt DL, et al. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. European Heart Journal 2021;42(14):1289-367. [DOI: 10.1093/eurheartj/ehaa575] - DOI - PubMed
Connolly 2009
-
- Connolly SJ, Ezekowitz MD, Yusuf S, Eikelboom J, Oldgren J, Parekh A, et al. Dabigatran versus warfarin in patients with atrial fibrillation. New England Journal of Medicine 2009;361(12):1139-51. - PubMed
Cuker 2019
-
- Cuker A, Burnett A, Triller D, Crowther M, Ansell J, Van Cott EM, et al. Reversal of direct oral anticoagulants: guidance from the Anticoagulation Forum. American Journal of Hematology 2019;94:697. - PubMed
Cutlip 2007
-
- Cutlip DE, Windecker S, Mehran R, Boam A, Cohen DJ, van Es G-A, et al. Clinical end points in coronary stent trials: a case for standardized definitions. Circulation 2007;115:2344-51. - PubMed
Deeks 2022
-
- Deeks JJ, Higgins JPT, Altman DG, editor(s). Chapter 10: Analysing data and undertaking meta-analyses. In: Higgins JP, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, Welch VA, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 6.3 (updated February 2022). Cochrane, 2022. Available from training.cochrane.org/handbook/archive/v.6.3.
Eriksson 2011
-
- Eriksson B, Quinlan DJ, Eikelboom JW. Novel oral factor Xa and thrombin inhibitors in the management of thromboembolism. Annual Review of Medicine 2011;62:41-57. - PubMed
Farag 2019
-
- Farag M, Spinthakis N, Gue YX, Srinivasan M, Sullivan K, Wellsted D, et al. Impaired endogenous fibrinolysis in ST-segment elevation myocardial infarction patients undergoing primary percutaneous coronary intervention is a predictor of recurrent cardiovascular events: the RISK PPCI study. European Heart Journal 2019;40(3):295-305. [DOI: 10.1093/eurheartj/ehy656] - DOI - PubMed
Garg 2015
-
- Garg P, Galper BZ, Cohen DJ, Yeh RW, Mauri L. Balancing the risks of bleeding and stent thrombosis: a decision analytic model to compare durations of dual antiplatelet therapy after drug-eluting stents. American Heart Journal 2015;169(2):222-33.e5. [DOI: 10.1016/j.ahj.2014.11.002] [PMID: ] - DOI - PMC - PubMed
Gibson 2011
-
- Gibson CM, Mega JL, Burton P, Goto S, Verheugt F, Bode C, et al. Rationale and design of the anti-Xa therapy to lower cardiovascular events in addition to standard therapy in subjects with acute coronary syndrome-thrombolysis in myocardial infarction 51 (ATLAS-ACS 2 TIMI 51) trial: a randomized, double-blind, placebo-controlled study to evaluate the efficacy and safety of rivaroxaban in subjects with acute coronary syndrome. American Heart Journal 2011;161(5):815-21. - PubMed
Giugliano 2013
-
- Giugliano RP, Ruff CT, Braunwald E, Murphy SA, Wiviott SD, Halperin JL, et al. Edoxaban versus warfarin in patients with atrial fibrillation. New England Journal of Medicine 2013;369(22):2093-104. - PubMed
Glund 2015
-
- Glund S, Moschetti V, Norris S, Stangier J, Schmohl M, Ryn J, et al. A randomised study in healthy volunteers to investigate the safety, tolerability and pharmacokinetics of idarucizumab, a specific antidote to dabigatran. Thrombosis and Haemostasis 2015;113(5):943-51. - PubMed
GRADEpro GDT 2015 [Computer program]
-
- GRADEpro GDT. Hamilton (ON): McMaster University (developed by Evidence Prime), 2015. Available at gradepro.org.
Granger 2011
-
- Granger CB, Alexander JH, McMurray JJ, Lopes RD, Hylek EM, Hanna M, et al. Apixaban versus warfarin in patients with atrial fibrillation. New England Journal of Medicine 2011;365(11):981-92. - PubMed
Higgins 2017
-
- Higgins JP, Altman DG, Sterne JA, editor(s). Chapter 8: Assessing risk of bias in included studies. In: Higgins JP, Churchill R, Chandler J, Cumpston MS, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 5.2.0 (updated June 2017). The Cochrane Collaboration, 2017. Available from training.cochrane.org/handbook/archive/v5.2.
Hurlen 2002
-
- Hurlen M, Abdelnoor M, Smith P, Erikssen J, Arnesen H. Warfarin, aspirin, or both after myocardial infarction. New England Journal of Medicine 2002;347:969-74. - PubMed
Ibanez 2018
-
- Ibanez B, James S, Agewall S, Antunes MJ, Bucciarelli-Ducci C, Bueno H, et al. 2017 ESC guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: the Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). European Heart Journal 2018;39(2):119-77. - PubMed
Jackson 2012
James 2018
-
- James SL, Abate D, Abate KH, Abay SM, Abbafati C, Abbasi N, et al. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018;392(10159):1789-858. - PMC - PubMed
Jan 2018
Jernberg 2015
-
- Jernberg T, Hasvold P, Henriksson M, Hjelm H, Thuresson M, Janzon M. Cardiovascular risk in post-myocardial infarction patients: nationwide real world data demonstrate the importance of a long-term perspective. European Heart Journal 2015;36(19):1163-70. - PubMed
Khan 2017
Kikkert 2018
Krahn 2013
Lefebvre 2022
-
- Lefebvre C, Glanville J, Briscoe S, Featherstone R, Littlewood A, Marshall C, et al. Chapter 4: Searching for and selecting studies. In: Higgins JP, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, Welch VA, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 6.3 (updated February 2022). Cochrane, 2022. Available from training.cochrane.org/handbook/archive/v.6.3.
Leon 1998
-
- Leon MB, Baim DS, Popma JJ, Gordon PC, Cutlip DE, Ho KK, et al. A clinical trial comparing three antithrombotic-drug regimens after coronary-artery stenting. New England Journal of Medicine 1998;339(23):1665-71. - PubMed
Liang 2020
-
- Liang L, Moore B, Soni A. National Inpatient Hospital Costs: The Most Expensive Conditions by Payer, 2017: Statistical Brief #261; July 2020. www.hcup-us.ahrq.gov/reports/statbriefs/sb261-Most-Expensive-Hospital-Co... (accessed 4 May 2021). - PubMed
Mega 2012
-
- Mega JL, Braunwald E, Wiviott SD, Bassand JP, Bhatt D, Bode C, et al. Rivaroxaban in patients with a recent acute coronary syndrome. New England Journal of Medicine 2012;366(1):9-19. - PubMed
Merlini 1994
-
- Merlini PA, Bauer KA, Oltrona L, Ardissino D, Cattaneo M, Belli C, et al. Persistent activation of coagulation mechanism in unstable angina and myocardial infarction. Circulation 1994;90(1):61-8. - PubMed
NICE 2015
-
- NICE. Rivaroxaban for prevention adverse outcomes after acute management of acute coronary syndrome. www.nice.org.uk/guidance/ta335/resources/rivaroxaban-for-preventing-adve... (accessed 28 April 2021).
O'Gara 2013
-
- O'Gara PT, Kushner FG, Ascheim DD, Casey DE, Chung MK, Lemos JA, et al. American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation 2013;127(4):e362-425. [DOI: 10.1161/CIR.0b013e3182742cf6] - DOI - PubMed
Oldgren 2011
-
- Oldgren J, Budaj A, Granger CB, Khder Y, Roberts J, Siegbahn A, et al. Dabigatran vs. placebo in patients with acute coronary syndromes on dual antiplatelet therapy: a randomized, double-blind, phase II trial. European Heart Journal 2011;32(22):2781-9. - PubMed
Oldgren 2013
Page 2021
Patel 2011
-
- Patel MR, Mahaffey KW, Garg J, Pan G, Singer DE, Hacke W, et al. Rivaroxaban versus warfarin in nonvalvular atrial fibrillation. New England Journal of Medicine 2011;365(10):883-91. - PubMed
Pollack 2015
-
- Pollack CV, Reilly PA, Eikelboom J, Glund S, Verhamme P, Bernstein RA, et al. Idarucizumab for dabigatran reversal. New England Journal of Medicine 2015;373(6):511-20. - PubMed
Review Manager 2020 [Computer program]
-
- Review Manager 5 (RevMan 5). Version 5.4. Copenhagen: Nordic Cochrane Centre, The Cochrane Collaboration, 2020.
Roffi 2016
-
- Roffi M, Patrono C, Collet JP, Mueller C, Valgimigli M, Andreotti F, et al. 2015 ESC guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: Task Force for the Management of Acute Coronary Syndromes in Patients Presenting Without Persistent ST-Segment Elevation of the European Society of Cardiology (ESC). European Heart Journal 2016;37(3):267-315. - PubMed
Rothberg 2005
-
- Rothberg MB, Celestin C, Fiore LD, Lawler E, Cook JR. Warfarin plus aspirin after myocardial infarction or the acute coronary syndrome: meta-analysis with estimates of risk and benefit. Annals of Internal Medicine 2005;143:241-50. - PubMed
Rücker 2012
-
- Rücker G. Network meta-analysis, electrical networks and graph theory. Research Synthesis Methods 2012;3(4):312-24. - PubMed
Rücker 2014
-
- Rücker G, Schwarzer G. Reduce dimension or reduce weights? Comparing two approaches to multi-arm studies in network meta-analysis. Statistics in Medicine 2014;33(25):4353-69. - PubMed
Rücker 2015
Rücker 2017
-
- Rücker G, Schwarzer G, Krahn U, König J. netmeta: Network Meta-Analysis using Frequentist Methods. cran.r-project.org/web/packages/netmeta (accessed 6 May 2021).
Saraf 2010
-
- Saraf S, Christopoulos C, Salha IB, Stott DJ, Gorog DA. Impaired endogenous thrombolysis in acute coronary syndrome patients predicts cardiovascular death and nonfatal myocardial infarction. Journal of the American College of Cardiology 2010;55:2107-15. - PubMed
Schünemann 2022
-
- Schünemann HJ, Higgins JPT, Vist GE, Glasziou P, Akl EA, Skoetz N, Guyatt GH. Chapter 14: Completing 'Summary of findings' tables and grading the certainty of the evidence. In: Higgins JP, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, Welch VA, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 6.3 (updated February 2022). Cochrane, 2022. Available from training.cochrane.org/handbook/archive/v.6.3.
Sumaya 2018a
Sumaya 2018b
Sumaya 2020
Valgimigli 2017
-
- Valgimigli M, Bueno H, Byrne RA, Collet JP, Costa F, Jeppsson A, et al. 2017 ESC focused update on dual antiplatelet therapy in coronary artery disease developed in collaboration with EACTS: the Task Force for dual antiplatelet therapy in coronary artery disease of the European Society of Cardiology (ESC) and of the European Association for Cardio-Thoracic Surgery (EACTS). European Heart Journal 2017;39(3):213-60. - PubMed
van Es 2002
-
- Es RF, Jonker JJ, Verheugt FW, Deckers JW, Grobbee DE. Antithrombotics in the Secondary Prevention of Events in Coronary Thrombosis-2 (ASPECT-2) research group. Aspirin and coumadin after acute coronary syndromes (the ASPECT-2 study): a randomised controlled trial. Lancet 2002;360:109-13. - PubMed
Varin 2013
-
- Varin R, Mirshahi S, Mirshahi P, Klein C, Jamshedov J, Chidiac J, et al. Whole blood clots are more resistant to lysis than plasma clots – greater efficacy of rivaroxaban. Thrombosis Research 2013;131:e100-9. - PubMed
Vos 2016
-
- Vos T, Allen C, Arora M, Barber RM, Bhutta ZA, Brown A, et al. Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990–2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016;388(10053):1545-602. - PMC - PubMed
Wilkins 2017
-
- Wilkins E, Wilson L, Wickramasinghe K, Bhatnagar P, Leal J, Luengo-Fernandez R, et al. European Cardiovascular Disease Statistics 2017. European Heart Network, Brussels.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical