

Stereotactic body radiotherapy plus rucosopasem in locally advanced or borderline resectable pancreatic cancer: GRECO-2 phase II study design
- PMID: 38264869
- PMCID: PMC10988540
- DOI: 10.2217/fon-2022-1219
Stereotactic body radiotherapy plus rucosopasem in locally advanced or borderline resectable pancreatic cancer: GRECO-2 phase II study design
Abstract
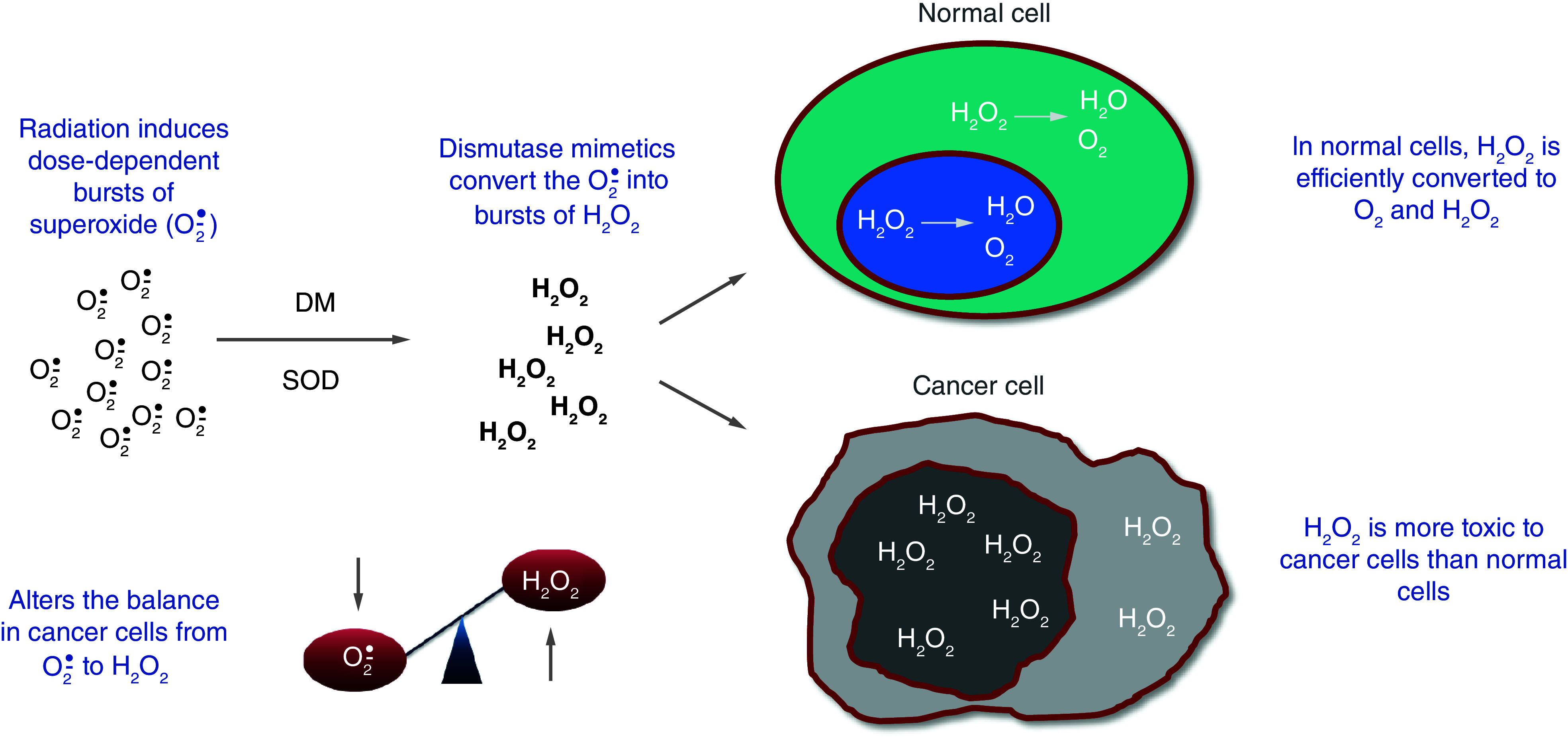
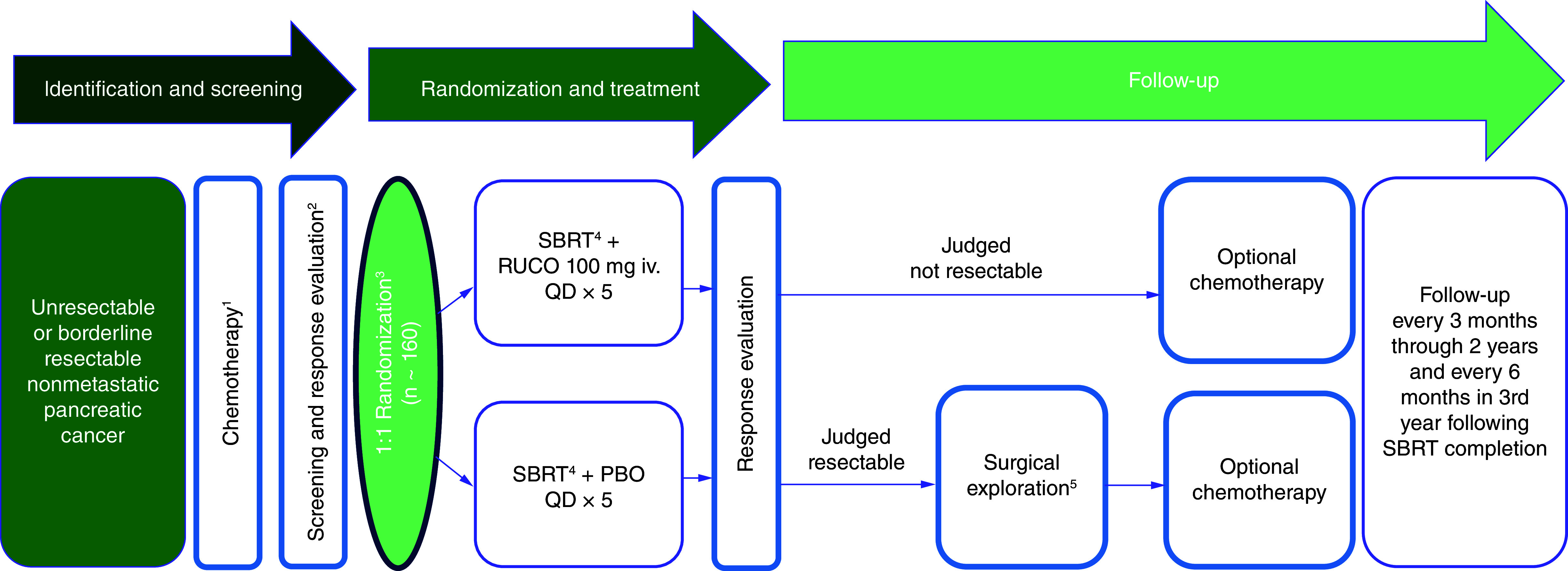
Ablative doses of stereotactic body radiotherapy (SBRT) may improve pancreatic cancer outcomes but may carry greater potential for gastrointestinal toxicity. Rucosopasem, an investigational selective dismutase mimetic that converts superoxide to hydrogen peroxide, can potentially increase tumor control of SBRT without compromising safety. GRECO-2 is a phase II, multicenter, randomized, double-blind, placebo-controlled trial of rucosopasem in combination with SBRT in locally advanced or borderline resectable pancreatic cancer. Patients will be randomized to rucosopasem 100 mg or placebo via intravenous infusion over 15 min, before each SBRT fraction (5 × 10 Gy). The primary end point is overall survival. Secondary end points include progression-free survival, locoregional control, time to metastasis, surgical resection rate, best overall response, in-field local response and acute and long-term toxicity.
Trial registration: ClinicalTrials.gov NCT04698915.
Keywords: pancreatic cancer; rucosopasem; stereotactic body radiation therapy; superoxide dismutase mimetic.
Plain language summary
The use of high doses of radiation delivered directly to tumors (stereotactic body radiation therapy [SBRT]) may improve survival compared with lower doses of radiation in patients with pancreatic cancer, but it may increase side effects. Rucosopasem, an investigational new drug being developed, can potentially improve the ability of SBRT to treat tumors without decreasing safety. In a previous study, median overall survival was improved when patients were treated with SBRT plus avasopasem, a drug that works the same way as rucosopasem. GRECO-2 is a clinical trial of rucosopasem used in combination with SBRT for treatment of localized pancreatic cancer. Patients will be randomly selected to receive either rucosopasem 100 mg or placebo via intravenous infusion over 15 min, before each SBRT treatment. The main result being studied is overall survival. Additional results include amount of time before tumors start to grow, how often patients get tumors surgically removed, best overall response and long-term safety. Clinical Trial Registration: NCT04698915 (ClinicalTrials.gov).
Conflict of interest statement
Competing interests disclosure
SE Hoffe reports employment with MyCareGorithm, has patents, royalties or other intellectual property from UpToDate, has other relationships with Beyond the White Coat, holds stock and other ownership interests from Rittenhouse Book Distributors, received honoraria from UpToDate; received research funding from Galera Therapeutics, Inc., and has uncompensated relationships with Galera Therapeutics, Inc. and ViewRay. TA Aguilera reports research funding from Apexigen and Galera Therapeutics, Inc., patents, royalties and other intellectual property from UCSD/ Avelas Biosciences and Stanford/AKSO Biosciences, honoraria from Apexigen and stock ownership with AKSO Biopharmaceutical and Avelas Biosciences. PJ Parikh reports speakers' fees, honoraria and institutional research funding from ViewRay, research funding from Galera Therapeutics, Inc., and stock ownership with Nuvaira. MM Ghaly reports institutional research funding from Galera Therapeutics, Inc. JM Herman reports research funding from 1440 for the Canopy Cancer Collective, travel and accommodations from Varian Medical Systems, honoraria from Boston Scientific, honoraria, stock, and other ownership interests from HistoSonics, and honoraria with MyCareGorithm. JM Caster reports institutional research funding from GSK and Galera Therapeutics, Inc. DW Kim reports research funding from Bold Therapeutics. James Costello reports honoraria from ViewRay and institutional research funding from Galera Therapeutics, Inc. MP Malafa reports research funding from Galera Therapeutics, Inc. Elizabeth C. Moser reports employment from Deka Biosciences, Inc, and advisory roles with Galera Therapeutics, Inc. EP Kennedy reports employment, leadership, and stock and other ownership interests from Galera Therapeutics, Inc. K Terry reports employment and stock with Galera Therapeutics, Inc. M Kurman reports consulting or advisory roles with Galera Therapeutics, Inc. The authors have no other competing interests or relevant affiliations with any organization or entity with the subject matter or materials discussed in the manuscript apart from those disclosed.
Figures
Similar articles
-
Stereotactic body radiotherapy with or without selective dismutase mimetic in pancreatic adenocarcinoma: an adaptive, randomised, double-blind, placebo-controlled, phase 1b/2 trial.Lancet Oncol. 2023 Dec;24(12):1387-1398. doi: 10.1016/S1470-2045(23)00478-3. Lancet Oncol. 2023. PMID: 38039992 Free PMC article. Clinical Trial.
-
Preoperative treatment with mFOLFIRINOX or Gemcitabine/Nab-paclitaxel +/- isotoxic high-dose stereotactic body Radiation Therapy (iHD-SBRT) for borderline resectable pancreatic adenocarcinoma (the STEREOPAC trial): study protocol for a randomised comparative multicenter phase II trial.BMC Cancer. 2023 Sep 21;23(1):891. doi: 10.1186/s12885-023-11327-x. BMC Cancer. 2023. PMID: 37735634 Free PMC article.
-
AGITG MASTERPLAN: a randomised phase II study of modified FOLFIRINOX alone or in combination with stereotactic body radiotherapy for patients with high-risk and locally advanced pancreatic cancer.BMC Cancer. 2021 Aug 19;21(1):936. doi: 10.1186/s12885-021-08666-y. BMC Cancer. 2021. PMID: 34412605 Free PMC article.
-
Conventionally fractionated radiation therapy versus stereotactic body radiation therapy for locally advanced pancreatic cancer (CRiSP): An international systematic review and meta-analysis.Cancer. 2020 May 15;126(10):2120-2131. doi: 10.1002/cncr.32756. Epub 2020 Mar 3. Cancer. 2020. PMID: 32125712
-
Maximizing Tumor Control and Limiting Complications With Stereotactic Body Radiation Therapy for Pancreatic Cancer.Int J Radiat Oncol Biol Phys. 2021 May 1;110(1):206-216. doi: 10.1016/j.ijrobp.2020.11.017. Epub 2020 Dec 24. Int J Radiat Oncol Biol Phys. 2021. PMID: 33358561 Review.
Cited by
-
Pharmacological ascorbate combined with rucosopasem selectively radio-chemo-sensitizes NSCLC via generation of H2O2.Redox Biol. 2025 Mar;80:103505. doi: 10.1016/j.redox.2025.103505. Epub 2025 Jan 23. Redox Biol. 2025. PMID: 39884000 Free PMC article.
References
-
- American Cancer Society. Cancer Facts & Figures 2023 (2023). Available at: www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statisti... (Accessed: 19 July 2023).
-
- Palta M, Godfrey D, Goodman KA et al. Radiation Therapy for Pancreatic Cancer: Executive Summary of an ASTRO Clinical Practice Guideline. Pract. Radiat. Oncol. 9(5), 322–332 (2019). - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical