

Indole-3-Propionic Acid Protects Against Heart Failure With Preserved Ejection Fraction
- PMID: 38264909
- PMCID: PMC10923103
- DOI: 10.1161/CIRCRESAHA.123.322381
Indole-3-Propionic Acid Protects Against Heart Failure With Preserved Ejection Fraction
Abstract
Background: Heart failure with preserved ejection fraction (HFpEF) is a common but poorly understood form of heart failure, characterized by impaired diastolic function. It is highly heterogeneous with multiple comorbidities, including obesity and diabetes, making human studies difficult.
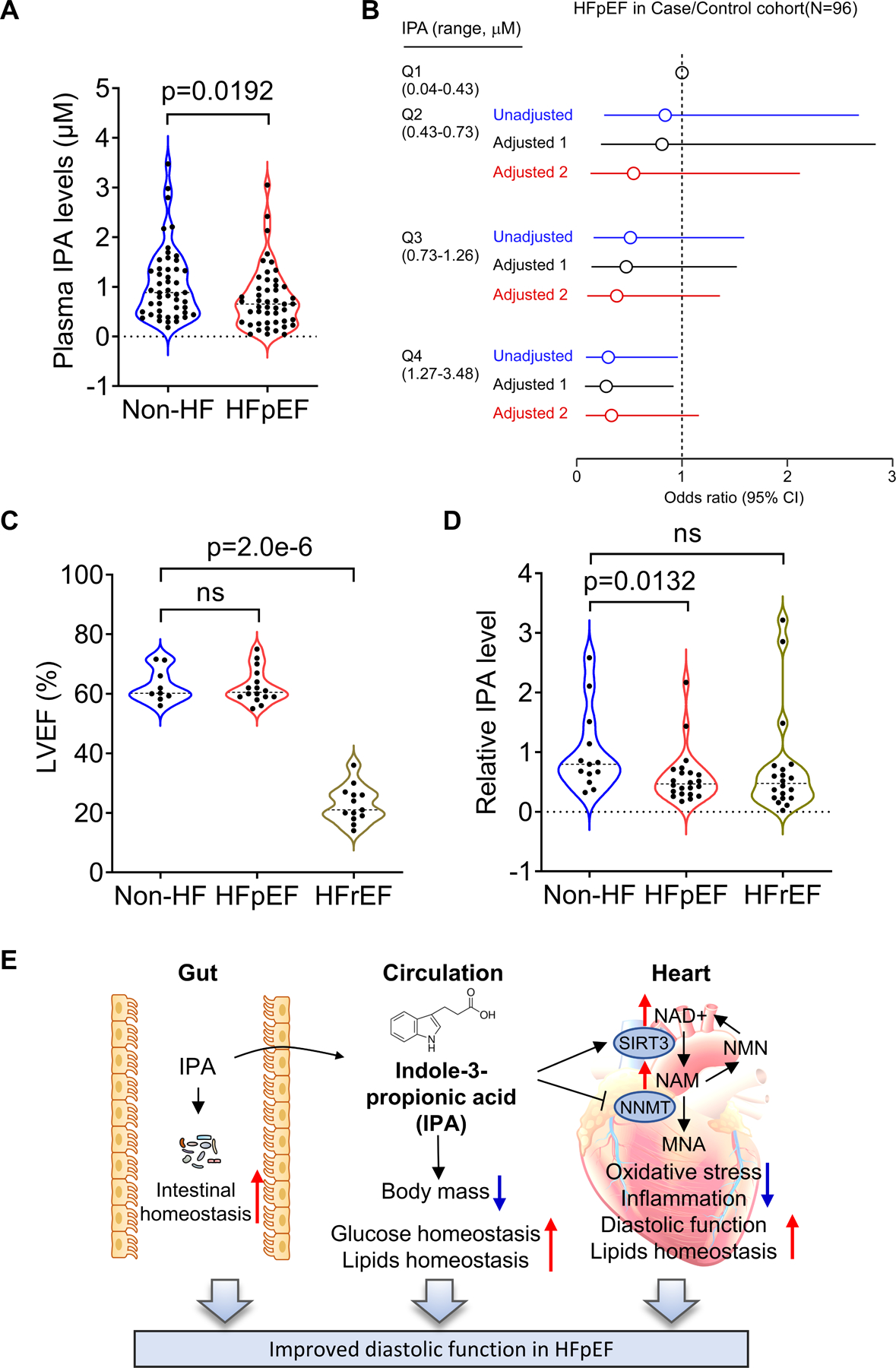
Methods: Metabolomic analyses in a mouse model of HFpEF showed that levels of indole-3-propionic acid (IPA), a metabolite produced by gut bacteria from tryptophan, were reduced in the plasma and heart tissue of HFpEF mice as compared with controls. We then examined the role of IPA in mouse models of HFpEF as well as 2 human HFpEF cohorts.
Results: The protective role and therapeutic effects of IPA were confirmed in mouse models of HFpEF using IPA dietary supplementation. IPA attenuated diastolic dysfunction, metabolic remodeling, oxidative stress, inflammation, gut microbiota dysbiosis, and intestinal epithelial barrier damage. In the heart, IPA suppressed the expression of NNMT (nicotinamide N-methyl transferase), restored nicotinamide, NAD+/NADH, and SIRT3 (sirtuin 3) levels. IPA mediates the protective effects on diastolic dysfunction, at least in part, by promoting the expression of SIRT3. SIRT3 regulation was mediated by IPA binding to the aryl hydrocarbon receptor, as Sirt3 knockdown diminished the effects of IPA on diastolic dysfunction in vivo. The role of the nicotinamide adenine dinucleotide circuit in HFpEF was further confirmed by nicotinamide supplementation, Nnmt knockdown, and Nnmt overexpression in vivo. IPA levels were significantly reduced in patients with HFpEF in 2 independent human cohorts, consistent with a protective function in humans, as well as mice.
Conclusions: Our findings reveal that IPA protects against diastolic dysfunction in HFpEF by enhancing the nicotinamide adenine dinucleotide salvage pathway, suggesting the possibility of therapeutic management by either altering the gut microbiome composition or supplementing the diet with IPA.
Keywords: NAD; heart failure, diastolic; microbiota; niacinamide; receptors, aryl hydrocarbon.
Conflict of interest statement
Figures







Comment in
-
From Gut to Heart: Role of Indole-3-Propionic Acid in HFpEF.Circ Res. 2024 Feb 16;134(4):390-392. doi: 10.1161/CIRCRESAHA.123.323947. Epub 2024 Feb 15. Circ Res. 2024. PMID: 38359099 No abstract available.
References
-
- Dunlay SM, Roger VL and Redfield MM. Epidemiology of heart failure with preserved ejection fraction. Nat Rev Cardiol 2017;14:591–602. - PubMed
-
- Iwano H and Little WC. Heart failure: what does ejection fraction have to do with it? J Cardiol 2013;62:1–3. - PubMed
-
- Owan TE, Hodge DO, Herges RM, Jacobsen SJ, Roger VL and Redfield MM. Trends in prevalence and outcome of heart failure with preserved ejection fraction. N Engl J Med 2006;355:251–9. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
