

A rare dissecting anterior inferior cerebellar artery aneurysm treated with flow diversion using a silk vista baby device
- PMID: 38264953
- PMCID: PMC11577331
- DOI: 10.1177/15910199241227467
A rare dissecting anterior inferior cerebellar artery aneurysm treated with flow diversion using a silk vista baby device
Abstract
Background: Dissecting intracranial pseudoaneurysms represent a challenge for treatment both endovascularly and surgically.
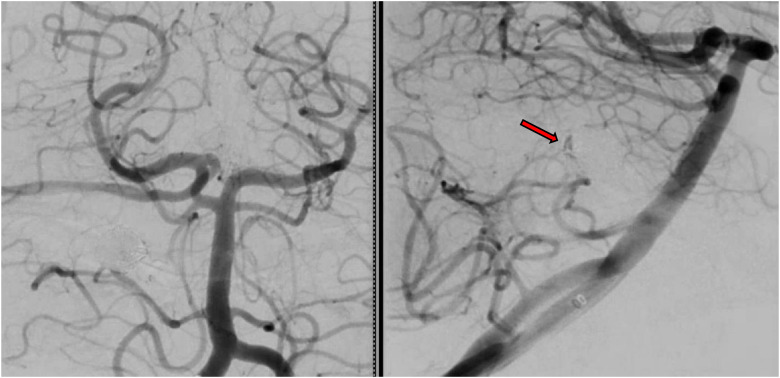
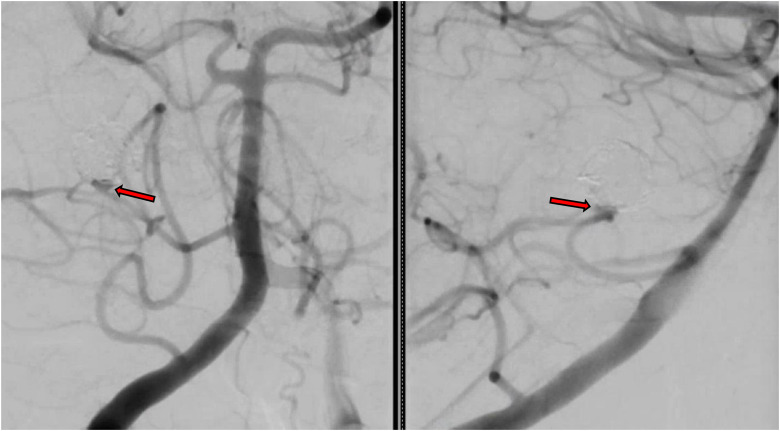
Methods: We review the treatment course of a ruptured anterior inferior cerebellar artery (AICA) dissecting pseudoaneurysm in a 50-year-old patient and review the history of dissecting aneurysms and AICA aneurysms treatment.
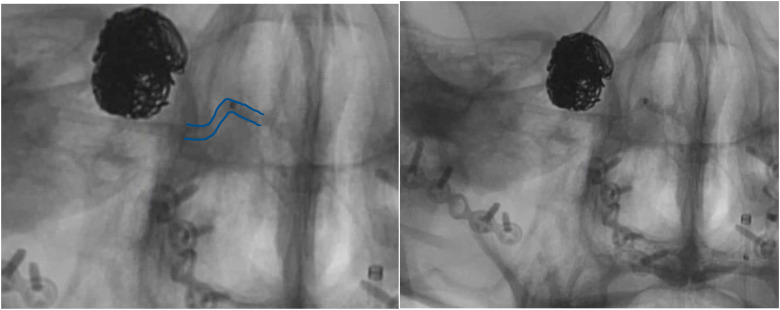
Results: An aneurysm cure was achieved using flow diversion in the AICA. The recent introduction of flow diversion devices that can be deployed through 0.017" microcatheters represents a new avenue for treatment of aneurysms.
Conclusion: To the best of our knowledge this is the first published case of flow diversion in the(?) AICA to treat a dissecting aneurysm. The introduction of Silk Vista Baby and similar future devices is likely to widen the scope of aneurysm treatment utilizing flow diversion in distal distribution with small parent arteries.
Keywords: Anterior inferior cerebellar artery; Silk Vista Baby; aneurysm; dissection; flow diversion.
Conflict of interest statement
Declaration of conflicting interestsThe authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures


















Similar articles
-
Flow diversion of a dissecting PICA aneurysm.Neurosurg Focus Video. 2022 Oct 1;7(2):V9. doi: 10.3171/2022.7.FOCVID2247. eCollection 2022 Oct. Neurosurg Focus Video. 2022. PMID: 36425264 Free PMC article.
-
Endovascular treatment for anterior inferior cerebellar artery-posterior inferior cerebellar artery (AICA-PICA) common trunk variant aneurysms: Technical note and literature review.J Cerebrovasc Endovasc Neurosurg. 2023 Dec;25(4):452-461. doi: 10.7461/jcen.2023.E2022.10.011. Epub 2023 Apr 12. J Cerebrovasc Endovasc Neurosurg. 2023. PMID: 37041684 Free PMC article.
-
[Four cases of direct surgery for anterior inferior cerebellar artery aneurysms].No Shinkei Geka. 2007 Jun;35(6):571-8. No Shinkei Geka. 2007. PMID: 17564050 Review. Japanese.
-
Occipital Artery to Anterior Inferior Cerebellar Artery (AICA) Bypass for Treatment of a Ruptured Proximal AICA-Posterior Inferior Cerebellar Artery Mycotic Aneurysm.World Neurosurg. 2020 Oct;142:176-178. doi: 10.1016/j.wneu.2020.06.090. Epub 2020 Jun 23. World Neurosurg. 2020. PMID: 32585380
-
[Trapping of ruptured dissecting aneurysm of distal anterior inferior cerebellar artery--case report].Brain Nerve. 2009 Feb;61(2):203-7. Brain Nerve. 2009. PMID: 19235471 Review. Japanese.
Cited by
-
Recovery of neurological complications following endovascular parent artery occlusion of ruptured a2 segment anterior inferior cerebellar artery aneurysm: a case report.Acta Neurochir (Wien). 2025 May 16;167(1):142. doi: 10.1007/s00701-025-06517-4. Acta Neurochir (Wien). 2025. PMID: 40377780 Free PMC article.
-
Difficulty and prospects of endovascular treatment for spontaneous intracranial artery dissection.Front Neurol. 2025 Mar 3;16:1560883. doi: 10.3389/fneur.2025.1560883. eCollection 2025. Front Neurol. 2025. PMID: 40098682 Free PMC article. Review.
References
-
- Ohkuma H, Suzuki S, Ogane K. Dissecting aneurysms of intracranial carotid circulation. Stroke 2002; 33: 941–947. - PubMed
-
- Kan P, Sweid A, Srivatsan Aet al. et al. Expanding indications for flow diverters: ruptured aneurysms, blister aneurysms, and dissecting aneurysms. Neurosurgery 2020; 86: S96–s103. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
