

Cost-Effectiveness of Screening Strategies for Familial Hypercholesterolaemia: An Updated Systematic Review
- PMID: 38265575
- PMCID: PMC10937756
- DOI: 10.1007/s40273-023-01347-7
Cost-Effectiveness of Screening Strategies for Familial Hypercholesterolaemia: An Updated Systematic Review
Abstract
Background: OBJECTIVE: This study aimed to systematically synthesise the cost-effectiveness of screening strategies to detect heterozygous familial hypercholesterolemia (FH).
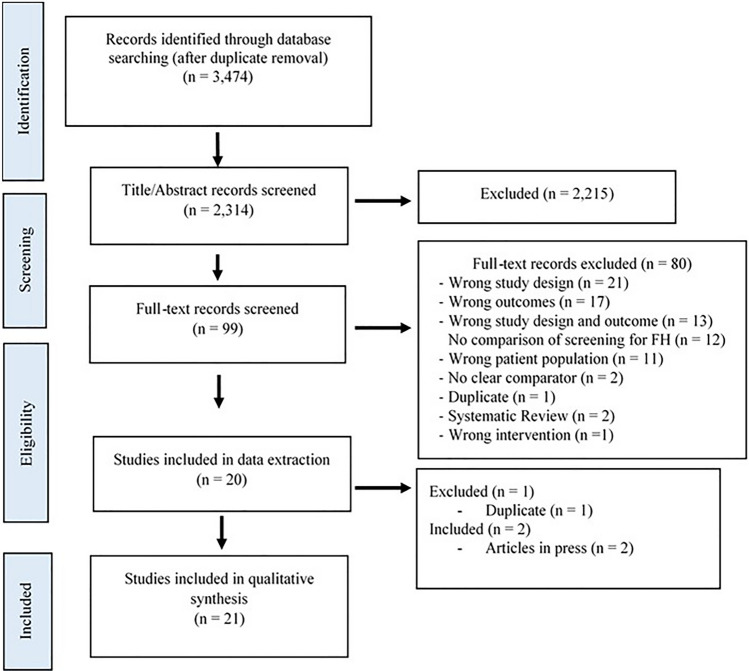
Methods: We searched seven databases from inception to 2 February , 2023, for eligible cost-effective analysis (CEA) that evaluated screening strategies for FH versus the standard care for FH detection. Independent reviewers performed the screening, data extraction and quality evaluation. Cost results were adapted to 2022 US dollars (US$) to facilitate comparisons between studies using the same screening strategies. Cost-effectiveness thresholds were based on the original study criteria.
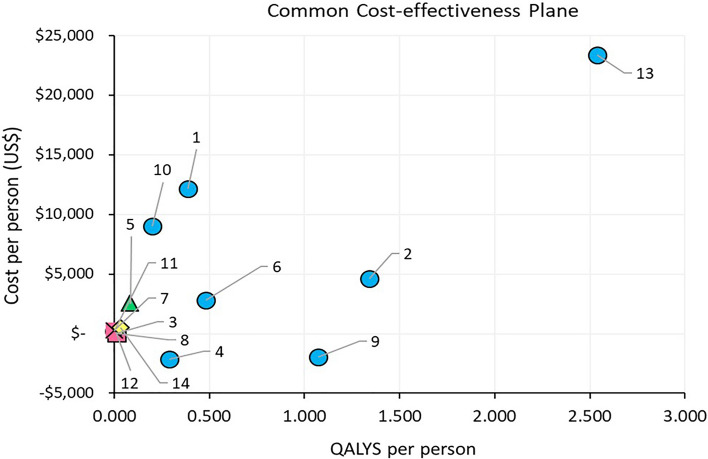
Results: A total of 21 studies evaluating 62 strategies were included in this review, most of the studies (95%) adopted a healthcare perspective in the base case, and majority were set in high-income countries. Strategies analysed included cascade screening (23 strategies), opportunistic screening (13 strategies), systematic screening (11 strategies) and population-wide screening (15 strategies). Most of the strategies relied on genetic diagnosis for case ascertainment. The most common comparator was no screening, but some studies compared the proposed strategy versus current screening strategies or versus the best next alternative. Six studies evaluated screening in children while the remaining were targeted at adults. From a healthcare perspective, cascade screening was cost-effective in 78% of the studies [cost-adapted incremental cost-effectiveness ratios (ICERs) ranged from dominant to 2022 US$ 104,877], opportunistic screening in 85% (ICERs from US$4959 to US$41,705), systematic screening in 80% (ICERs from US$2763 to US$69,969) and population-wide screening in 60% (ICERs from US$1484 to US$223,240). The most common driver of ICER identified in the sensitivity analysis was the long-term cost of lipid-lowering treatment.
Conclusions: Based on reported willingness to pay thresholds for each setting, most CEA studies concluded that screening for FH compared with no screening was cost-effective, regardless of the screening strategy. Cascade screening resulted in the largest health benefits per person tested.
© 2024. The Author(s).
Conflict of interest statement
DA, YB, TA, AL and PD report no conflict of interest. CM, JIM, ML and ZA are authors in some of the studies included in this systematic review; no other conflict of interest. GFW reports honoraria for lectures and advisory boards or research grants from Amgen, outside the submitted work.
Figures
Similar articles
-
Synthesized economic evidence on the cost-effectiveness of screening familial hypercholesterolemia.Glob Health Res Policy. 2024 Sep 26;9(1):38. doi: 10.1186/s41256-024-00382-x. Glob Health Res Policy. 2024. PMID: 39327612 Free PMC article.
-
Cost-effectiveness of universal genetic screening for familial hypercholesterolemia in young adults aged 18-40 years in China.BMC Med. 2025 Mar 5;23(1):139. doi: 10.1186/s12916-025-03966-7. BMC Med. 2025. PMID: 40045404 Free PMC article.
-
Universal screening at age 1-2 years as an adjunct to cascade testing for familial hypercholesterolaemia in the UK: A cost-utility analysis.Atherosclerosis. 2018 Aug;275:434-443. doi: 10.1016/j.atherosclerosis.2018.05.047. Epub 2018 Jun 4. Atherosclerosis. 2018. PMID: 29937236
-
Probabilistic cost-effectiveness analysis of cascade screening for familial hypercholesterolaemia using alternative diagnostic and identification strategies.Heart. 2011 Jul;97(14):1175-81. doi: 10.1136/hrt.2010.213975. Heart. 2011. PMID: 21685482
-
Genetic Testing for Familial Hypercholesterolemia: Health Technology Assessment.Ont Health Technol Assess Ser. 2022 Aug 23;22(3):1-155. eCollection 2022. Ont Health Technol Assess Ser. 2022. PMID: 36158868 Free PMC article.
Cited by
-
Screening for Familial Hypercholesterolemia in Children and its Cost-Effectiveness.J Atheroscler Thromb. 2025 Aug 1;32(8):926-928. doi: 10.5551/jat.ED285. Epub 2025 Jun 5. J Atheroscler Thromb. 2025. PMID: 40467520 Free PMC article. No abstract available.
-
A Cost-Effectiveness Analysis for the Combination of Universal Screening at 9-10 Years Old and Reverse Cascade Screening of Relatives for Familial Hypercholesterolemia in Japan.J Atheroscler Thromb. 2025 Aug 1;32(8):962-981. doi: 10.5551/jat.65181. Epub 2025 Feb 14. J Atheroscler Thromb. 2025. PMID: 39956559 Free PMC article.
-
Synthesized economic evidence on the cost-effectiveness of screening familial hypercholesterolemia.Glob Health Res Policy. 2024 Sep 26;9(1):38. doi: 10.1186/s41256-024-00382-x. Glob Health Res Policy. 2024. PMID: 39327612 Free PMC article.
-
A qualitative study of perceptions of the care pathway for familial hypercholesterolemia: screening, diagnosis, treatment, and family cascade screening.Implement Sci Commun. 2024 Dec 2;5(1):135. doi: 10.1186/s43058-024-00670-0. Implement Sci Commun. 2024. PMID: 39623509 Free PMC article.
-
The Power of the Pedigree: Cascade Screening in Familial Hypercholesterolemia.JACC Adv. 2024 Aug 13;3(9):101201. doi: 10.1016/j.jacadv.2024.101201. eCollection 2024 Sep. JACC Adv. 2024. PMID: 39247676 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
