

Long-Term Outcomes after Conversion to a Belatacept-Based Immunosuppression in Kidney Transplant Recipients
- PMID: 38265815
- PMCID: PMC11108246
- DOI: 10.2215/CJN.0000000000000411
Long-Term Outcomes after Conversion to a Belatacept-Based Immunosuppression in Kidney Transplant Recipients
Abstract
Background: Conversion to a belatacept-based immunosuppression is currently used as a calcineurin inhibitor (CNI) avoidance strategy when the CNI-based standard-of-care immunosuppression is not tolerated after kidney transplantation. However, there is a lack of evidence on the long-term benefit and safety after conversion to belatacept.
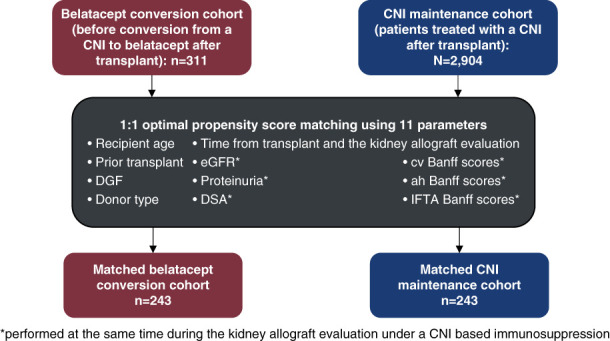
Methods: We prospectively enrolled 311 kidney transplant recipients from 2007 to 2020 from two referral centers, converted from CNI to belatacept after transplant according to a prespecified protocol. Patients were matched at the time of conversion to patients maintained with CNIs, using optimal matching. The primary end point was death-censored allograft survival at 7 years. The secondary end points were patient survival, eGFR, and safety outcomes, including serious viral infections, immune-related complications, antibody-mediated rejection, T-cell-mediated rejection, de novo anti-HLA donor-specific antibody, de novo diabetes, cardiovascular events, and oncologic complications.
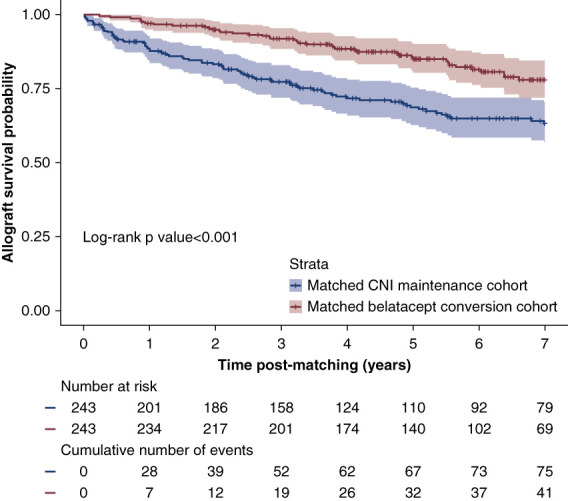
Results: A total of 243 patients converted to belatacept (belatacept group) were matched to 243 patients maintained on CNIs (CNI control group). All recipient, transplant, functional, histologic, and immunologic parameters were well balanced between the two groups with a standardized mean difference below 0.05. At 7 years post-conversion to belatacept, allograft survival was 78% compared with 63% in the CNI control group ( P < 0.001 for log-rank test). The safety outcomes showed a similar rate of patient death (28% in the belatacept group versus 36% in the CNI control group), active antibody-mediated rejection (6% versus 7%), T-cell-mediated rejection (4% versus 4%), major adverse cardiovascular events, and cancer occurrence (9% versus 11%). A significantly higher rate of de novo proteinuria was observed in the belatacept group as compared with the CNI control group (37% versus 21%, P < 0.001).
Conclusions: This real-world evidence study shows that conversion to belatacept post-transplant was associated with lower risk of graft failure and acceptable safety outcomes compared with patients maintained on CNIs.
Clinical trial registry name and registration number: Long-term Outcomes after Conversion to Belatacept, NCT04733131 .
Copyright © 2024 by the American Society of Nephrology.
Conflict of interest statement
D. Anglicheau reports consultancy for BMS, Chiesi, and Sandoz; honoraria from Astellas, AstraZeneca, BMS, Chiesi, Novartis, and Sandoz; and patents pending (EP21305960.3 and EP 2021060415). O. Aubert received a grant from the Bettencourt Schueller Foundation. O. Aubert also reports honoraria from CareDX and Novartis. G. Divard received a grant from the French Foundation for Medical Research and the French Speaking Society of Nephrology, Dialysis, and Transplantation. G. Divard also reports employment with Paris Institute for Transplantation and Organ Regeneration, INSERM U970. C. Lefaucheur reports serving as a scientific advisor and board member of Predict4Health. C. Legendre reports honoraria from Alexion, Astellas, Novartis, and Sandoz and speakers bureau for Hansa Medical. A. Loupy received financial support from INSERM-Action thématique incitative sur programme Avenir (ATIP-Avenir), RHU KTDInnov (17-RHUS-0010) and H2020 EUTRAIN (No. 754995). A. Loupy also reports employment with Paris Institute for Transplantation and Organ Regeneration, ownership interest in Cibiltech, research funding from BMS, and honoraria from BMS. A. Loupy reports employment with Paris Institute for Transplantation and Organ Regeneration, ownership interest in Cibiltech, research funding from BMS, and honoraria from BMS. All remaining authors have nothing to disclose.
Figures

References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
