

A Prospective Multicenter ≥2 Years Clinical Study of the Active Apex Correction (APC) Technique in Early Onset Scoliosis (EOS) Patients
- PMID: 38266098
- PMCID: PMC11571920
- DOI: 10.1177/21925682241229677
A Prospective Multicenter ≥2 Years Clinical Study of the Active Apex Correction (APC) Technique in Early Onset Scoliosis (EOS) Patients
Abstract
Study design: prospective multicenter study.
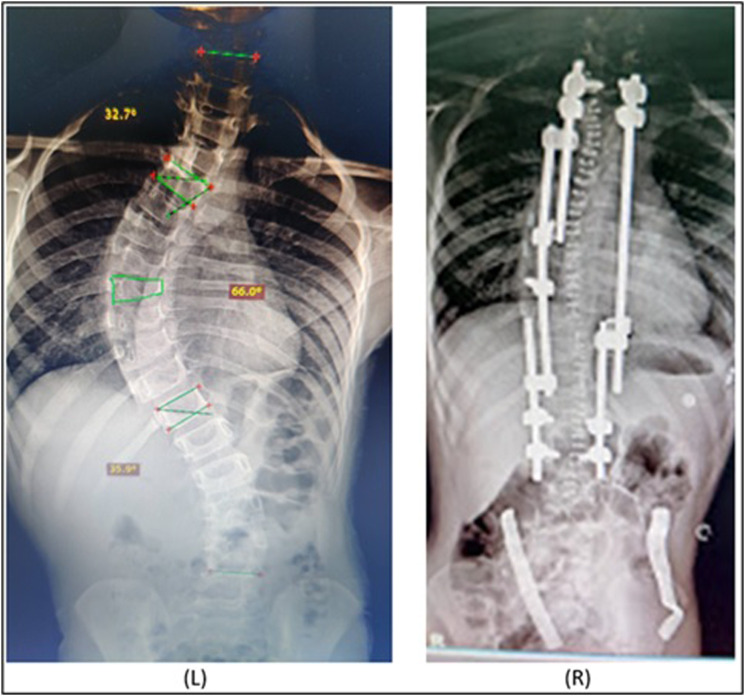
Objectives: Active apex correction (APC) is posterior tethering technique for correction of early onset scoliosis (EOS) via reverse modulation at the apex. Active apex correction has been increasingly used worldwide. This study aimed to assess short-term outcomes of multicenter study with ≥2 years of APC on spine length, curve correction, complications, unplanned surgeries, and proposed low crankshaft phenomena incidence.
Methods: Prospective multicenter study including 24 EOS patients treated by APC; involves inserting and compressing pedicle screws on convex side of apex proximal and distal to most wedged vertebra allowing apex modulation according to Hueter-Volkmann law. Excluded patients with <2 years follow-up whom APC was not primary surgery.
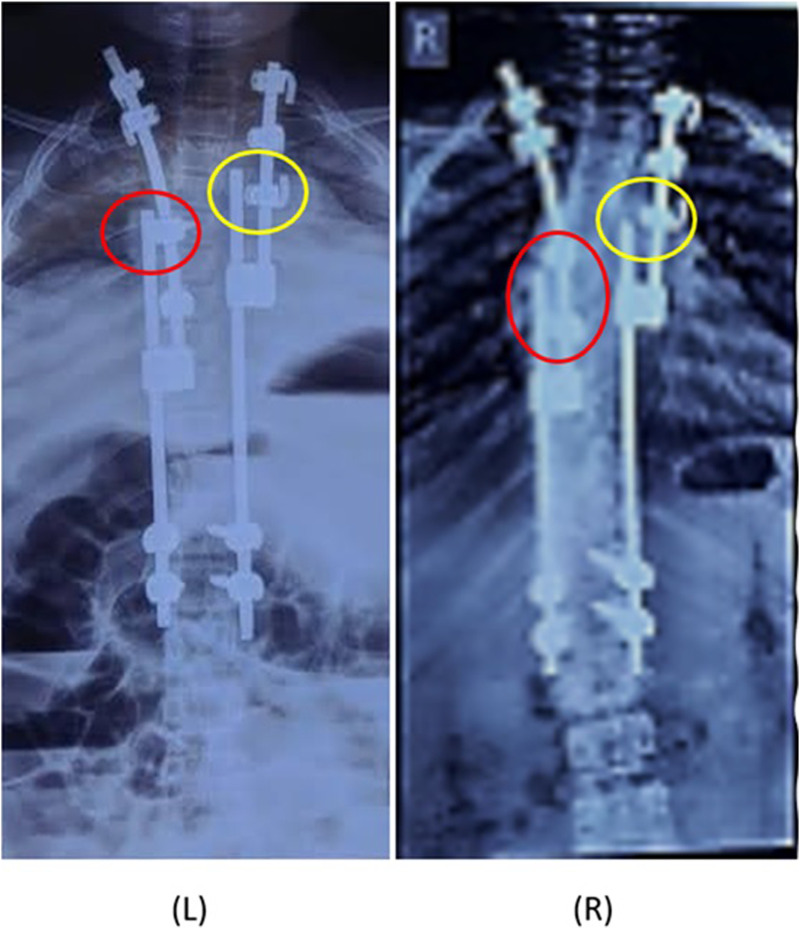
Results: Mean age 85.97 ± 32.43 months, 71% congenital scoliosis, mean follow-up 35.54 ± 12.36 months. At final follow-up, statistically significant improvement in Cobbs angle (∆ = 23.96%, P < .0001), spinal length T1-T12 (∆ = 12.83%, P < .0001), T1-L5 (∆ = 13.41%, P < .0001) but not in apical vertebral translation (AVT) albeit clinical improvement (∆ = 7.9%, P = .36) compared to preoperative measurements. Comparing immediate postoperative measurements to >2 years follow-up, statistically significant improvement in spinal length T1-T12 (∆ = 6.03%, P = .0002) and T1-L5 (∆ = 6.26%, P < .0001) but not in Cobbs angle (∆ = 4.93%, P = .3) or AVT (∆ = 14.77%, P = .25). 9 complications requiring 3 unplanned surgeries recorded in all patients including 2 broken rods, 2 adding-on and 4 screw dislodgement.
Conclusion: Active apex correction is a novel technique that has been incorporated in several countries as treatment modality for EOS. Short-term outcomes are promising in terms of clinical improvement, complication rates and decreased need for multiple operations or unplanned surgeries.
Keywords: active apex correction; apical vertebral translation; crankshafting; early onset scoliosis; spine correction.
Conflict of interest statement
Declaration of Conflicting InterestsThe author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: AA discloses consultancy from Tria Spine, consultancy from Proximie, Committee chair at SICOT, Committee member at SRS, NASS, AO spine. The rest of the authors have nothing to disclose.
Figures







References
-
- Schlösser T, Kruyt M, Tsirikos A. Surgical management of early-onset scoliosis: indications and currently available techniques. Orthopaedics and Trauma. 2021;35(6):336-346.
-
- Williams BA, Matsumoto H, McCalla DJ, et al. Development and initial validation of the classification of early-onset scoliosis (C-EOS). J Bone Joint Surg Am. 2014;96:1359e67. - PubMed
-
- Kim G, Sammak SE, Michalopoulos GD, et al. Comparison of surgical interventions for the treatment of early-onset scoliosis: a systematic review and meta-analysis. J Neurosurg Pediatr. 2022;31(4):342-357. - PubMed
-
- Skaggs DL, Guillaume T, El-Hawary R, Emans J, Mendelow M, Smith J. Early onset scoliosis Consensus Statement, SRS growing spine committee, 2015. Spine Deformity 2015;3:107.
LinkOut - more resources
Full Text Sources
Miscellaneous
