

Scoring donor lungs for graft failure risk: The Lung Donor Risk Index (LDRI)
- PMID: 38266712
- PMCID: PMC11939009
- DOI: 10.1016/j.ajt.2024.01.022
Scoring donor lungs for graft failure risk: The Lung Donor Risk Index (LDRI)
Abstract
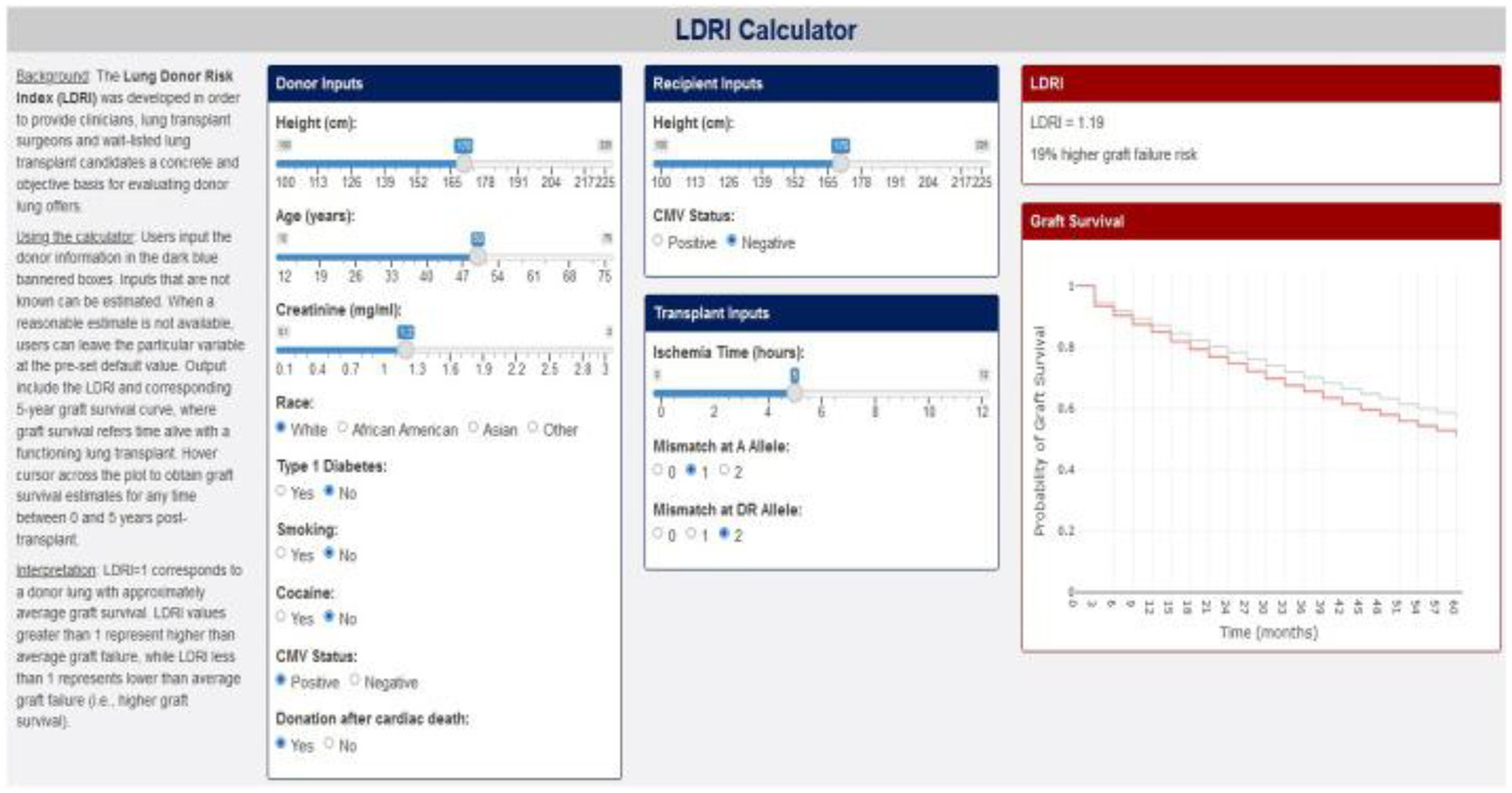
Lung transplantation lags behind other solid organ transplants in donor lung utilization due, in part, to uncertainty regarding donor quality. We sought to develop an easy-to-use donor risk metric that, unlike existing metrics, accounts for a rich set of donor factors. Our study population consisted of n = 26 549 adult lung transplant recipients abstracted from the United Network for Organ Sharing Standard Transplant Analysis and Research file. We used Cox regression to model graft failure (GF; earliest of death or retransplant) risk based on donor and transplant factors, adjusting for recipient factors. We then derived and validated a Lung Donor Risk Index (LDRI) and developed a pertinent online application (https://shiny.pmacs.upenn.edu/LDRI_Calculator/). We found 12 donor/transplant factors that were independently predictive of GF: age, race, insulin-dependent diabetes, the difference between donor and recipient height, smoking, cocaine use, cytomegalovirus seropositivity, creatinine, human leukocyte antigen (HLA) mismatch, ischemia time, and donation after circulatory death. Validation showed the LDRI to have GF risk discrimination that was reasonable (C = 0.61) and higher than any of its predecessors. The LDRI is intended for use by transplant centers, organ procurement organizations, and regulatory agencies and to benefit patients in decision-making. Unlike its predecessors, the proposed LDRI could gain wide acceptance because of its granularity and similarity to the Kidney Donor Risk Index.
Keywords: deceased-donor; graft failure; lung transplantation; risk prediction.
Copyright © 2024. Published by Elsevier Inc.
Figures




Similar articles
-
The UK DCD Risk Score: A new proposal to define futility in donation-after-circulatory-death liver transplantation.J Hepatol. 2018 Mar;68(3):456-464. doi: 10.1016/j.jhep.2017.10.034. Epub 2017 Nov 15. J Hepatol. 2018. PMID: 29155020
-
Lung Quality and Utilization in Controlled Donation After Circulatory Determination of Death Within the United States.Am J Transplant. 2016 Apr;16(4):1207-15. doi: 10.1111/ajt.13599. Epub 2016 Feb 4. Am J Transplant. 2016. PMID: 26844673 Free PMC article.
-
Decision making in liver transplantation--limited application of the liver donor risk index.Liver Transpl. 2014 Jul;20(7):831-7. doi: 10.1002/lt.23879. Liver Transpl. 2014. PMID: 24692309 Free PMC article.
-
Development of organ-specific donor risk indices.Liver Transpl. 2012 Apr;18(4):395-404. doi: 10.1002/lt.23398. Liver Transpl. 2012. PMID: 22287036 Free PMC article. Review.
-
Selecting lung transplant candidates: where do current guidelines fall short?Expert Rev Respir Med. 2012 Feb;6(1):51-61. doi: 10.1586/ers.11.83. Expert Rev Respir Med. 2012. PMID: 22283579 Free PMC article. Review.
Cited by
-
Impact of donor-recipient ethnic matching on survival after lung transplantation in Italy.Updates Surg. 2025 Aug 25. doi: 10.1007/s13304-025-02371-2. Online ahead of print. Updates Surg. 2025. PMID: 40855035
-
Differential effects of donor factors on post-transplant survival in lung transplantation.JHLT Open. 2024 Jul 1;5:100122. doi: 10.1016/j.jhlto.2024.100122. eCollection 2024 Aug. JHLT Open. 2024. PMID: 40143895 Free PMC article.
-
Lung Donation and Transplant Recipient Outcomes at Independent vs Hospital-Based Donor Care Units.JAMA Netw Open. 2024 Jun 3;7(6):e2417107. doi: 10.1001/jamanetworkopen.2024.17107. JAMA Netw Open. 2024. PMID: 38916893 Free PMC article.
References
-
- Snell GI, Yusen RD, Weill D, et al. Report of the ISHLT Working Group on Primary Lung Graft Dysfunction, part I: Definition and grading-A 2016 Consensus Group statement of the International Society for Heart and Lung Transplantation. J Heart Lung Transplant 2017;36(10):1097–1103. (In eng). DOI: 10.1016/j.healun.2017.07.021. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
