

Demographic, clinical, biomarker, and neuropathological correlates of posterior cortical atrophy: an international cohort study and individual participant data meta-analysis
- PMID: 38267189
- PMCID: PMC11615965
- DOI: 10.1016/S1474-4422(23)00414-3
Demographic, clinical, biomarker, and neuropathological correlates of posterior cortical atrophy: an international cohort study and individual participant data meta-analysis
Erratum in
-
Correction to Lancet Neurol 2024; 23: 168-77.Lancet Neurol. 2024 Apr;23(4):e8. doi: 10.1016/S1474-4422(24)00075-9. Epub 2024 Feb 13. Lancet Neurol. 2024. PMID: 38364829 No abstract available.
Abstract
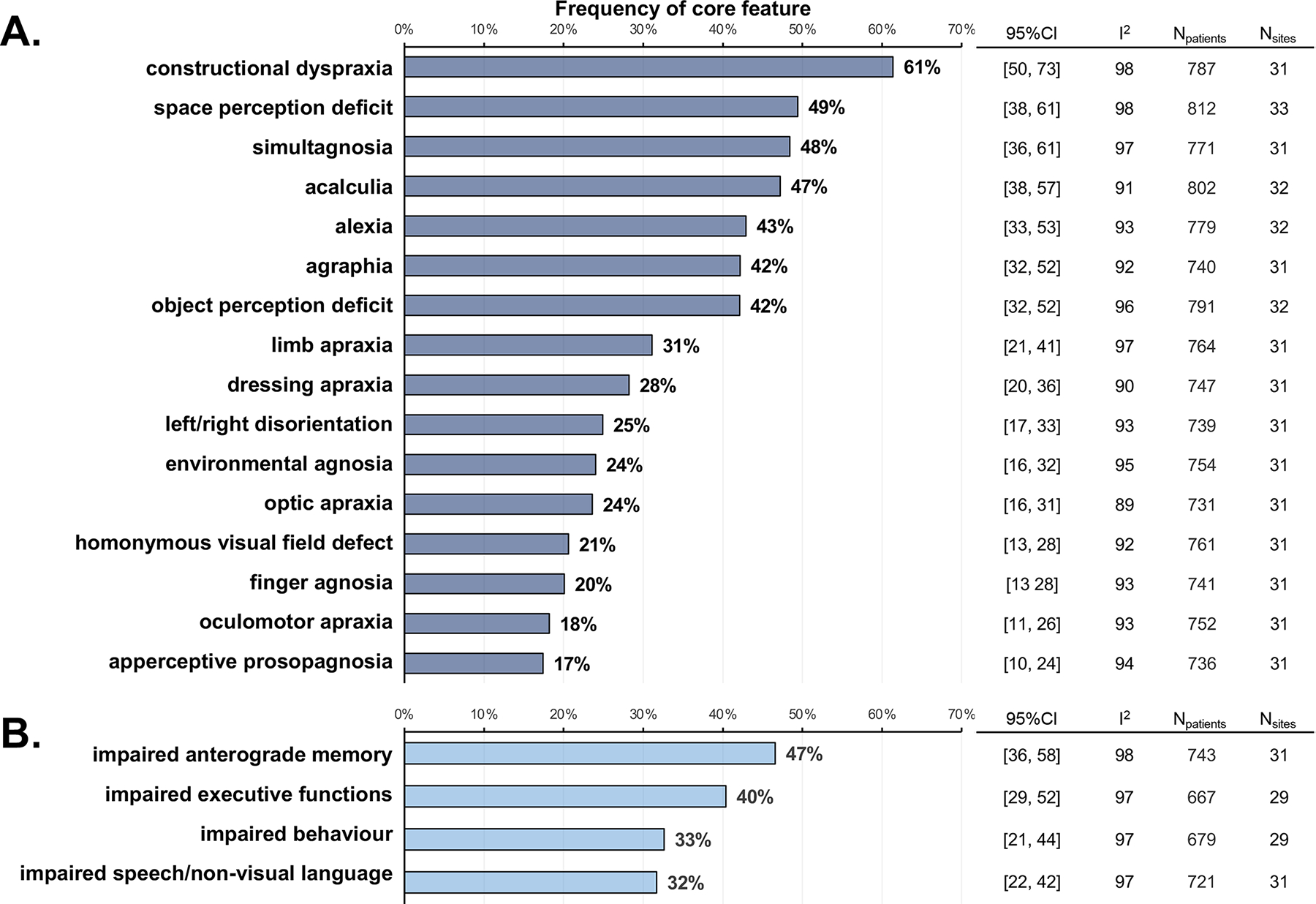
Background: Posterior cortical atrophy is a rare syndrome characterised by early, prominent, and progressive impairment in visuoperceptual and visuospatial processing. The disorder has been associated with underlying neuropathological features of Alzheimer's disease, but large-scale biomarker and neuropathological studies are scarce. We aimed to describe demographic, clinical, biomarker, and neuropathological correlates of posterior cortical atrophy in a large international cohort.
Methods: We searched PubMed between database inception and Aug 1, 2021, for all published research studies on posterior cortical atrophy and related terms. We identified research centres from these studies and requested deidentified, individual participant data (published and unpublished) that had been obtained at the first diagnostic visit from the corresponding authors of the studies or heads of the research centres. Inclusion criteria were a clinical diagnosis of posterior cortical atrophy as defined by the local centre and availability of Alzheimer's disease biomarkers (PET or CSF), or a diagnosis made at autopsy. Not all individuals with posterior cortical atrophy fulfilled consensus criteria, being diagnosed using centre-specific procedures or before development of consensus criteria. We obtained demographic, clinical, biofluid, neuroimaging, and neuropathological data. Mean values for continuous variables were combined using the inverse variance meta-analysis method; only research centres with more than one participant for a variable were included. Pooled proportions were calculated for binary variables using a restricted maximum likelihood model. Heterogeneity was quantified using I2.
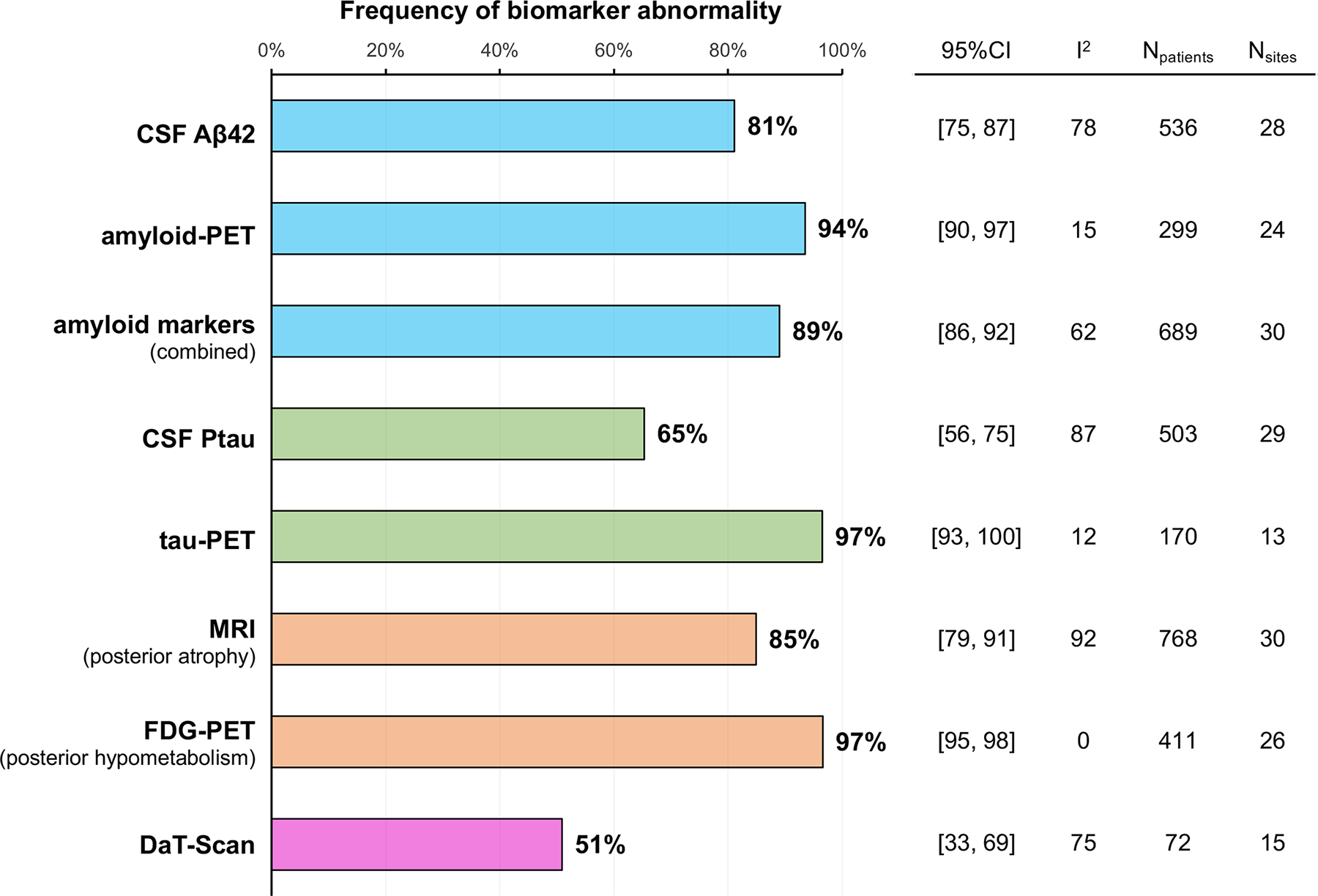
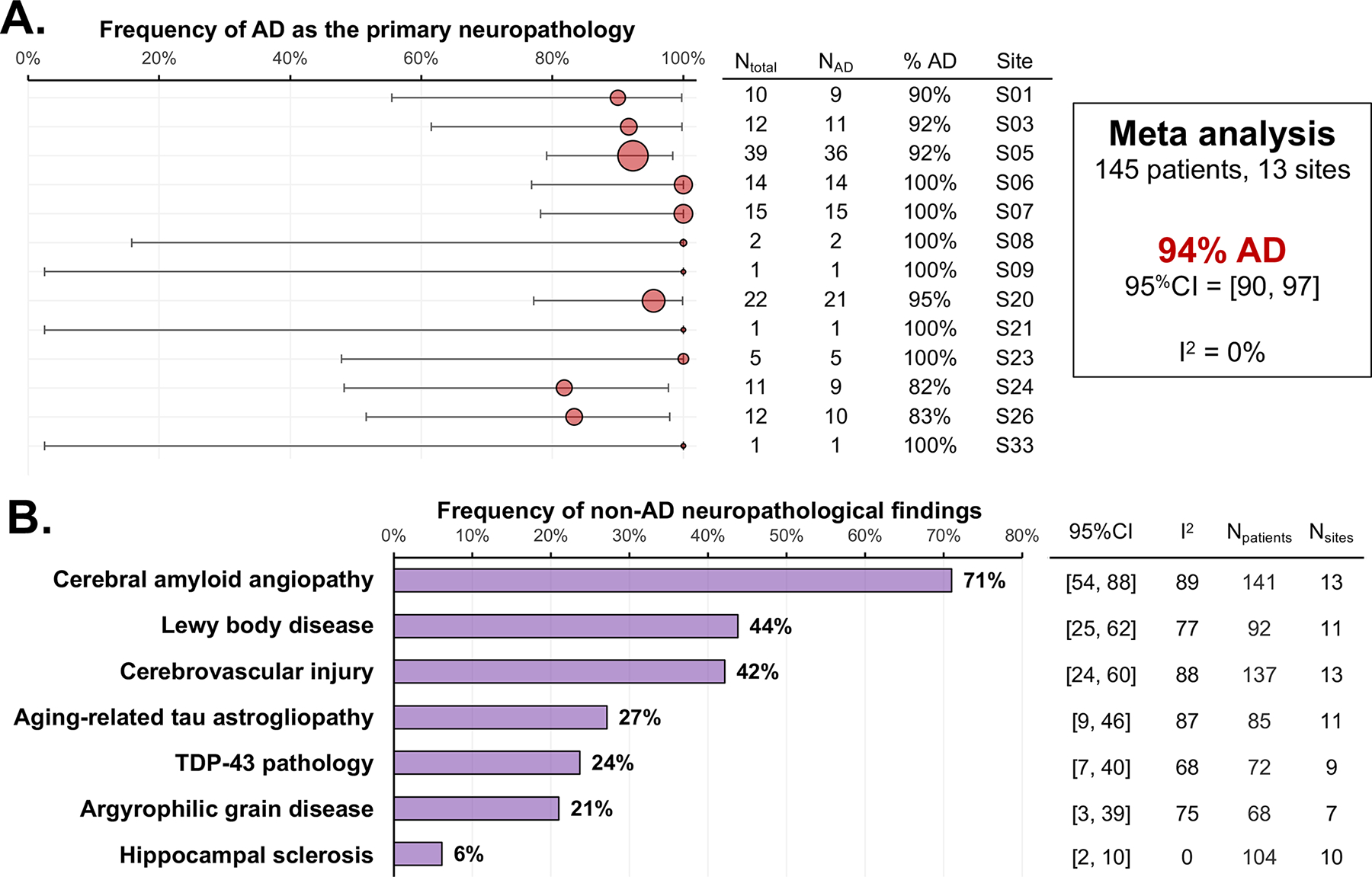
Findings: We identified 55 research centres from 1353 papers, with 29 centres responding to our request. An additional seven centres were recruited by advertising via the Alzheimer's Association. We obtained data for 1092 individuals who were evaluated at 36 research centres in 16 countries, the other sites having not responded to our initial invitation to participate to the study. Mean age at symptom onset was 59·4 years (95% CI 58·9-59·8; I2=77%), 60% (56-64; I2=35%) were women, and 80% (72-89; I2=98%) presented with posterior cortical atrophy pure syndrome. Amyloid β in CSF (536 participants from 28 centres) was positive in 81% (95% CI 75-87; I2=78%), whereas phosphorylated tau in CSF (503 participants from 29 centres) was positive in 65% (56-75; I2=87%). Amyloid-PET (299 participants from 24 centres) was positive in 94% (95% CI 90-97; I2=15%), whereas tau-PET (170 participants from 13 centres) was positive in 97% (93-100; I2=12%). At autopsy (145 participants from 13 centres), the most frequent neuropathological diagnosis was Alzheimer's disease (94%, 95% CI 90-97; I2=0%), with common co-pathologies of cerebral amyloid angiopathy (71%, 54-88; I2=89%), Lewy body disease (44%, 25-62; I2=77%), and cerebrovascular injury (42%, 24-60; I2=88%).
Interpretation: These data indicate that posterior cortical atrophy typically presents as a pure, young-onset dementia syndrome that is highly specific for underlying Alzheimer's disease pathology. Further work is needed to understand what drives cognitive vulnerability and progression rates by investigating the contribution of sex, genetics, premorbid cognitive strengths and weaknesses, and brain network integrity.
Funding: None.
Copyright © 2024 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests MC received research support from the Fonds de Recherche du Québec–Santé (FRQS). MF, FA, EC, FC, and GM receive research support from the Foundation Research on Alzheimer Disease and Italian Ministry of Healthy (#GR-2010-2303035). MEM receives research support from the NIH (R01 AG054449, R01 AG075802, U01-AG057195 and P30 AG062677). Data from Mayo Clinic (Jacksonville) was supported by the State of Florida Alzheimer's Disease Initiative and the Mayo Clinic Alzheimer's Disease Research Center. BD receives research funding from NIA R21-AG051987, P50-AG005134, and R01-DC014296 and philanthropic funding to the MGH FTD Unit including the Mooney Family Fund. KY is an Etherington posterior cortical atrophy Senior Research Fellow and is funded by the Alzheimer's Society, grant number 453 (AS-JF-18-003). The work was also supported by an Alzheimer's Research UK Senior Research Fellowship and ESRC/NIHR (ES/L001810/1) grant to SC. JMS acknowledges the support of the National Institute for Health Research University College London Hospitals Biomedical Research Centre, ARUK (ARUK-PG2017–1946), Weston Brain Institute (UB170045), Medical Research Council, and British Heart Foundation. TL is supported by an Alzheimer's Research UK senior fellowship. The Queen Square Brain Bank is supported by the Reta Lila Weston Institute for Neurological Studies and the Medical Research Council. The Dementia Research Centre is supported by Alzheimer's Research UK, Brain Research Trust, and The Wolfson Foundation. This work was also supported by the NIHR Queen Square Dementia Biomedical Research Unit, and the NIHR UCL/H Biomedical Research Centre. This work was supported by the MRC Dementia Platform UK and the UK Dementia Research Institute at UCL, which receives its funding from UK DRI, funded by the UK Medical Research Council, Alzheimer's Society and Alzheimer's Research UK. DG, AH, and GL receive research support from Shiley-Marcos ADRC P30 AG062429. KJ, JW, and JGR receive research funding from the NIH (R01-AG50603). BDCB receives funding from Alzheimer Nederland (#WE.15-2019-13, WE.03-2021-15, and #WE.06-2023-01). MM, JR, and KA were supported by the NIHR Cambridge Biomedical Research Centre including the Cambridge Brain Bank (BRC-1215-20014. The views expressed are those of the authors and not necessarily those of the NIHR or the Department of Health and Social Care) and the Race Against Dementia. M.F.M. receives research support from the NIA (1RF1AG050967). RM is supported by France Alzheimer, Fondation Recherche Alzheimer, Philippe Chatrier Foundation and by Rosita Gomez Association. OH has acquired research support (for the institution) from ADx, AVID Radiopharmaceuticals, Biogen, Eli Lilly, Eisai, Fujirebio, GE Healthcare, Pfizer, and Roche and has received consultancy or speaker fees from AC Immune, Amylyx, Alzpath, BioArctic, Biogen, Cerveau, Fujirebio, Genentech, Novartis, Roche, and Siemens. Work at the Lund University was supported by the Swedish Research Council (2016-00906), the Knut and Alice Wallenberg foundation (2017-0383), the Marianne and Marcus Wallenberg foundation (2015·0125), the Strategic Research Area MultiPark (Multidisciplinary Research in Parkinson's disease) at Lund University, the Swedish Alzheimer Foundation (AF-939932), the Swedish Brain Foundation (FO2021-0293), The Parkinson foundation of Sweden (1280/20), the Konung Gustaf V:s och Drottning Victorias Frimurarestiftelse, the Skåne University Hospital Foundation (2020-O000028), Regionalt Forskningsstöd (2020-0314), and the Swedish federal Government under the ALF agreement (2018-Projekt0279). PN is supported by The Mater Foundation. DP, SPC, and GT are supported by The Italian Ministry of Health (Ricerca Finalizzata Progetto Reti Nazionale AD NET-2011-02346784). OP, NC, JB, JH, and DF were supported by funding to ForeFront, a collaborative research group dedicated to the study of frontotemporal dementia and motor neuron disease, from the National Health and Medical Research Council (NHMRC) (GNT1037746) and the Australian Research Council (ARC) Centre of Excellence in Cognition and its Disorders Memory Program (CE11000102). OP is supported by an NHMRC Leadership Fellowship (GNT2008020). LA receives research support from Indiana Alzheimer's Disease Research Center (P30 AG010133 and LEADS (U01AG6057195). ER, SW, and MM received research support from the NIH (P30AG13854 and P30AG072977). BDCB receives funding from Alzheimer Nederland (#WE.15-2019-13, WE.03-2021-15, and #WE.06-2023-01). Data from Geneva was supported by Alzheimer's Disease Research Center (ADRC) grants (NIA P50 AG005138 and P30 AG066514). Data from Xuanwu Hospital was supported by the National Natural Science Foundation of China (81971011) and Beijing Municipal Science and Technology Committee (7202060). Research of Alzheimer Center Amsterdam has been funded by ZonMW, NWO, EU-FP7, EU-JPND, Alzheimer Nederland, Hersenstichting CardioVascular Onderzoek Nederland, Health Holland, Topsector Life Sciences & Health, stichting Dioraphte, Gieskes-Strijbis fonds, stichting Equilibrio, Edwin Bouw fonds, Pasman stichting, stichting Alzheimer & Neuropsychiatrie Foundation, Philips, Biogen MA, Novartis-NL, Life-MI, AVID, Roche BV, Fujifilm, and Combinostics. Data from Penn Frontotemporal Degeneration Center was funded by NIH grants (R01-AG054519 and K01-AG061277). Data from MASS's group comes from The Sant Pau Initiative on Neurodegeneration cohort. LTG receives research support from the NIH (K24053435) and R01AG075802. GDR receives research support from the NIH/NIA (R35 AG072362, P30-AG062422, U01-AG057195, and P01-AG019724). Other support to GDR includes National Institute of Neurological Disorders and Stroke, Alzheimer's Association, American College of Radiology, Rainwater Charitable Foundation, Shanendoah Foundation, Avid Radiopharmaceuticals, GE Healthcare, Life Molecular Imaging, and Genentech. LA has received personal compensation for serving as a consultant for Biogen, Two Labs, FL Dept Health, Genentech, NIH Biobank, Eli Lilly, GE Healthcare, Eisai, and Roche Diagnostics and for serving on a Data Safety and Monitoring Board for IQVIA. LA receives research support from the National Institute on Aging, the Alzheimer's Association, Roche Diagnostics, AVID radiopharmaceuticals, Life Molecular Imaging, and Eli Lilly. MFM is the section editor for Behavioral Neurology for UpToDate. JGR serves on the Drug Safety Monitoring Board for the National Institute of Neurological Disorders and Stroke StrokeNET. KAJ is an Associate Editor for Annals of Clinical and Translational Neurology and is on the editorial boards of Journal of Neurology, Acta Neuropathologica, and Neuropathology and Applied Neurobiology. JLW is an Associate Editor for Brain Connectivity and Journal of Alzheimer's Disease. RO has received research support from Avid Radiopharmaceuticals, has given lectures in symposia sponsored by GE Healthcare and is an editorial board member of Alzheimer's Research & Therapy and the European Journal of Nuclear Medicine and Molecular Imaging. FA is Associate Editor of NeuroImage: Clinical, has received speaker honoraria from Biogen Idec, Italfarmaco, Roche and Zambon, and receives or has received research supports from the Italian Ministry of Health, the Italian Ministry of University and Research, AriSLA (Fondazione Italiana di Ricerca per la SLA), and the European Research Council and Foundation Research on Alzheimer Disease. MF is Editor-in-Chief of the Journal of Neurology, Associate Editor of Human Brain Mapping, Neurological Sciences, and Radiology; received compensation for consulting services from Alexion, Almirall, Biogen, Merck, Novartis, Roche, and Sanofi; speaking activities from Bayer, Biogen, Celgene, Chiesi Italia SpA, Eli Lilly, Genzyme, Janssen, Merck-Serono, Neopharmed Gentili, Novartis, Novo Nordisk, Roche, Sanofi, Takeda, and TEVA; participation in Advisory Boards for Alexion, Biogen, Bristol-Myers Squibb, Merck, Novartis, Roche, Sanofi, Sanofi-Aventis, Sanofi-Genzyme, and Takeda; scientific direction of educational events for Biogen, Merck, Roche, Celgene, Bristol-Myers Squibb, Lilly, Novartis, and Sanofi-Genzyme; and receives research support from Biogen Idec, Merck-Serono, Novartis, Roche, Italian Ministry of Health, and Fondazione Italiana Sclerosi Multipla. GDR has served on Scientific Advisory Boards for Alector, Eli Lilly, Genentech, Merck, and Roche. He serves on a Data Safety and Monitoring Board for Johnson & Johnson. He is an Associate Editor for JAMA Neurology. The other authors declare no competing interests.
Figures
Comment in
-
Posterior cortical atrophy: new insights into treatments and biomarkers for Alzheimer's disease.Lancet Neurol. 2024 Feb;23(2):127-128. doi: 10.1016/S1474-4422(23)00501-X. Lancet Neurol. 2024. PMID: 38267172 No abstract available.
References
-
- Tang-Wai DF, Graff-Radford NR, Boeve BF, et al. Clinical, genetic, and neuropathologic characteristics of posterior cortical atrophy. Neurology 2004; 63(7): 1168–74. - PubMed
-
- Alladi S, Xuereb J, Bak T, et al. Focal cortical presentations of Alzheimer’s disease. Brain 2007; 130(Pt 10): 2636–45. - PubMed
-
- Renner JA, Burns JM, Hou CE, McKeel DW, Jr., Storandt M, Morris JC. Progressive posterior cortical dysfunction: a clinicopathologic series. Neurology 2004; 63(7): 1175–80. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- P30 AG013854/AG/NIA NIH HHS/United States
- R01 DC014296/DC/NIDCD NIH HHS/United States
- P30 AG010133/AG/NIA NIH HHS/United States
- U01 AG057195/AG/NIA NIH HHS/United States
- K24 AG053435/AG/NIA NIH HHS/United States
- P30 AG062422/AG/NIA NIH HHS/United States
- K01 AG061277/AG/NIA NIH HHS/United States
- P30 AG072976/AG/NIA NIH HHS/United States
- P30 AG066514/AG/NIA NIH HHS/United States
- R21 AG051987/AG/NIA NIH HHS/United States
- R01 AG054449/AG/NIA NIH HHS/United States
- R01 AG075802/AG/NIA NIH HHS/United States
- RF1 AG050967/AG/NIA NIH HHS/United States
- P30 AG062429/AG/NIA NIH HHS/United States
- P01 AG019724/AG/NIA NIH HHS/United States
- P50 AG005134/AG/NIA NIH HHS/United States
- R01 AG073282/AG/NIA NIH HHS/United States
- R35 AG072362/AG/NIA NIH HHS/United States
- P30 AG066546/AG/NIA NIH HHS/United States
- P50 AG005138/AG/NIA NIH HHS/United States
- P30 AG072977/AG/NIA NIH HHS/United States
- P30 AG062677/AG/NIA NIH HHS/United States
- R01 AG054519/AG/NIA NIH HHS/United States
- R01 AG050603/AG/NIA NIH HHS/United States
