

The combined effect of systemic antibiotics and proton pump inhibitors on Clostridioides difficile infection and recurrence
- PMID: 38267263
- PMCID: PMC10904719
- DOI: 10.1093/jac/dkae012
The combined effect of systemic antibiotics and proton pump inhibitors on Clostridioides difficile infection and recurrence
Abstract
Background: Antibiotics and proton pump inhibitors (PPI) are recognized risk factors for acquisition and recurrence of Clostridioides difficile infection (CDI), yet combined effects remain unclear.
Objectives: To assess the short- and long-term effects of antibiotics and PPIs on CDI risk and recurrence.
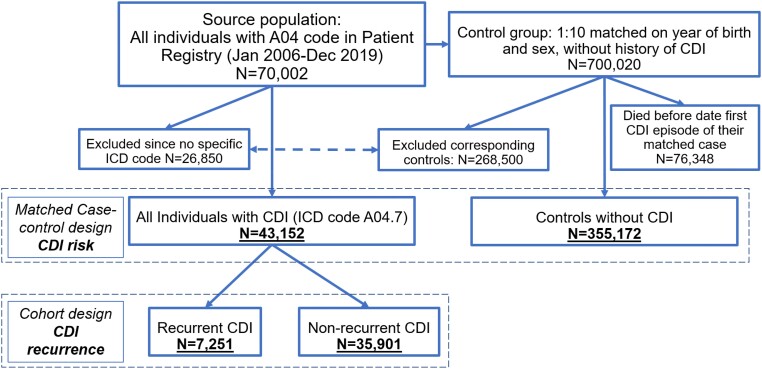
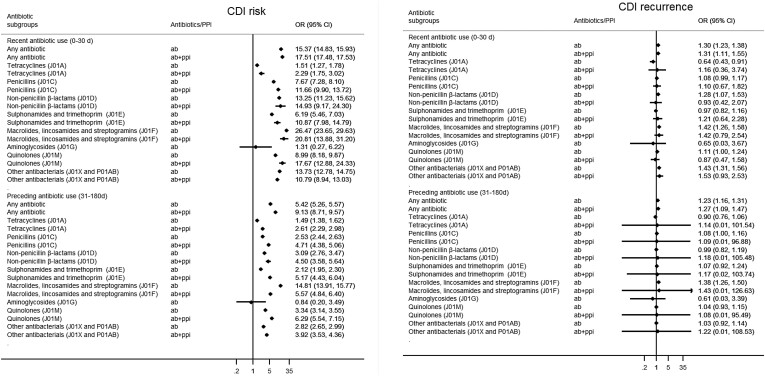
Methods: Population-based study including all 43 152 patients diagnosed with CDI in Sweden (2006-2019), and 355 172 matched population controls without CDI. The impact of antibiotics and PPIs on CDI risk and recurrence was explored for recent (0-30 days) and preceding (31-180 days) use prior to their first CDI diagnosis, using multivariable conditional logistic regression presented as odds ratios (ORs) and 95% confidence interval, adjusted for demographics, comorbidities and other drugs.
Results: Compared to controls, the combined effect of recent PPIs and antibiotics [ORAB+PPI = 17.51 (17.48-17.53)] on CDI risk was stronger than the individual effects [ORAB = 15.37 (14.83-15.93); ORPPI = 2.65 (2.54-2.76)]. Results were less pronounced for exposure during the preceding months. Dose-response analyses showed increasing exposure correlated with CDI risk [recent use: ORAB = 6.32 (6.15-6.49); ORPPI = 1.65 (1.62-1.68) per prescription increase].Compared to individuals without recurrence (rCDI), recent [ORAB = 1.30 (1.23-1.38)] and preceding [ORAB = 1.23 (1.16-1.31); ORPPI = 1.12 (1.03-1.21)] use also affected the risk of recurrence yet without significant interaction between both. Recent macrolides/lincosamides/streptogramins; other antibacterials including nitroimidazole derivates; non-penicillin beta lactams and quinolones showed the strongest association with CDI risk and recurrence, particularly for recent use. PPI use, both recent and preceding, further increased the CDI risk associated with almost all antibiotic classes.
Conclusion: Recent and less recent use of PPIs and systemic antibiotics was associated with an increased risk of CDI, particularly in combination.
© The Author(s) 2024. Published by Oxford University Press on behalf of British Society for Antimicrobial Chemotherapy.
Figures
Similar articles
-
Proton pump inhibitors and risk for recurrent Clostridium difficile infection among inpatients.Am J Gastroenterol. 2013 Nov;108(11):1794-801. doi: 10.1038/ajg.2013.333. Epub 2013 Sep 24. Am J Gastroenterol. 2013. PMID: 24060760 Free PMC article.
-
Incidence of Clostridium difficile infection in patients receiving high-risk antibiotics with or without a proton pump inhibitor.J Hosp Infect. 2016 Feb;92(2):173-7. doi: 10.1016/j.jhin.2015.10.009. Epub 2015 Nov 2. J Hosp Infect. 2016. PMID: 26616410
-
Proton Pump Inhibitors Do Not Increase Risk for Clostridium difficile Infection in the Intensive Care Unit.Am J Gastroenterol. 2016 Nov;111(11):1641-1648. doi: 10.1038/ajg.2016.343. Epub 2016 Aug 30. Am J Gastroenterol. 2016. PMID: 27575714 Free PMC article.
-
Magnitude and direction of the association between Clostridium difficile infection and proton pump inhibitors in adults and pediatric patients: a systematic review and meta-analysis.J Gastroenterol. 2018 Jan;53(1):84-94. doi: 10.1007/s00535-017-1369-3. Epub 2017 Jul 25. J Gastroenterol. 2018. PMID: 28744822
-
Risk of Clostridium difficile infection with acid suppressing drugs and antibiotics: meta-analysis.Am J Gastroenterol. 2012 Jul;107(7):1011-9. doi: 10.1038/ajg.2012.108. Epub 2012 Apr 24. Am J Gastroenterol. 2012. PMID: 22525304
Cited by
-
Proton Pump Inhibitor Use and Risk of Clostridioides difficile Infection: An Umbrella Review of 11 Meta-Analyses.Cureus. 2025 Jul 6;17(7):e87383. doi: 10.7759/cureus.87383. eCollection 2025 Jul. Cureus. 2025. PMID: 40765605 Free PMC article. Review.
-
A Comprehensive 10-Year Nationwide Pharmacovigilance Surveillance on Antibacterial Agents in Korea: Data Mining for Signal Detection of Trends and Seriousness of Adverse Events.Microorganisms. 2025 Jan 10;13(1):136. doi: 10.3390/microorganisms13010136. Microorganisms. 2025. PMID: 39858904 Free PMC article.
-
Recent advances in therapeutic probiotics: insights from human trials.Clin Microbiol Rev. 2025 Jun 12;38(2):e0024024. doi: 10.1128/cmr.00240-24. Epub 2025 Apr 22. Clin Microbiol Rev. 2025. PMID: 40261032 Review.
-
Clostridioides difficile infection, recurrence and the associated healthcare consumption in Sweden between 2006 and 2019: a population-based cohort study.BMC Infect Dis. 2024 May 3;24(1):468. doi: 10.1186/s12879-024-09364-3. BMC Infect Dis. 2024. PMID: 38702635 Free PMC article.
-
Presence of Drug Interaction Between Penicillin and Hormonal Contraceptives in Women: A Scoping Review.Healthcare (Basel). 2025 Jun 6;13(12):1364. doi: 10.3390/healthcare13121364. Healthcare (Basel). 2025. PMID: 40565391 Free PMC article. Review.
