

The prognostic value of radiological and pathological lymph node status in patients with cervical cancer who underwent neoadjuvant chemotherapy and followed hysterectomy
- PMID: 38267449
- PMCID: PMC10808453
- DOI: 10.1038/s41598-023-49539-7
The prognostic value of radiological and pathological lymph node status in patients with cervical cancer who underwent neoadjuvant chemotherapy and followed hysterectomy
Abstract
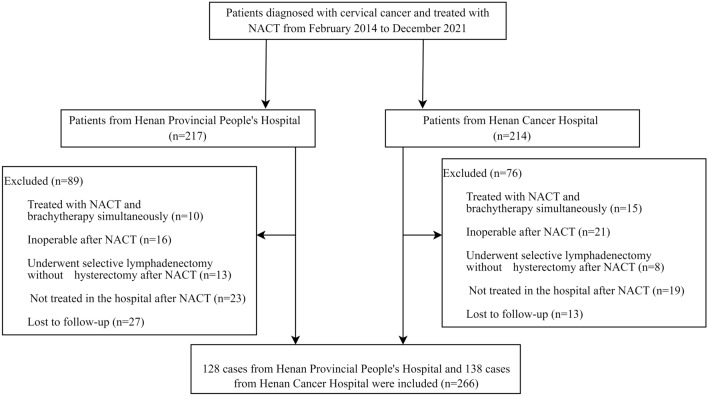
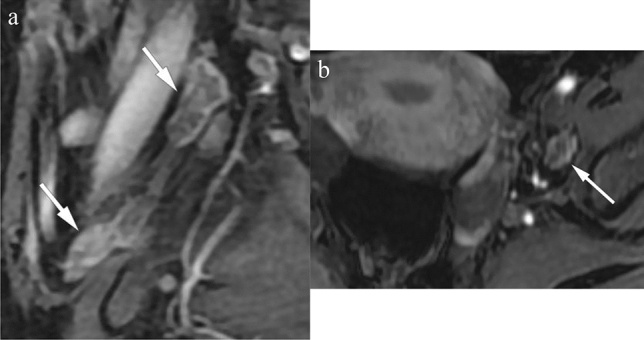
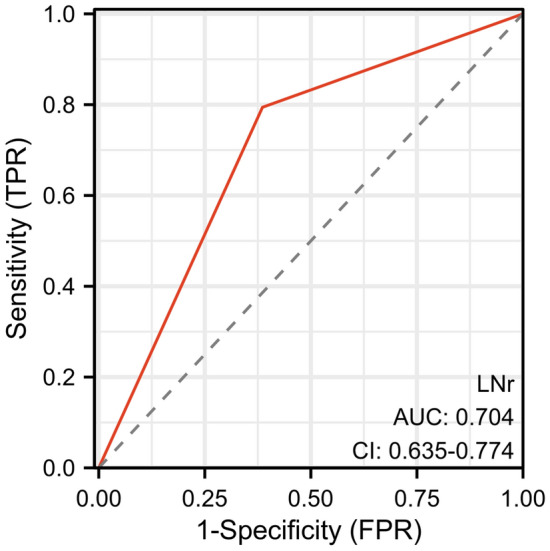
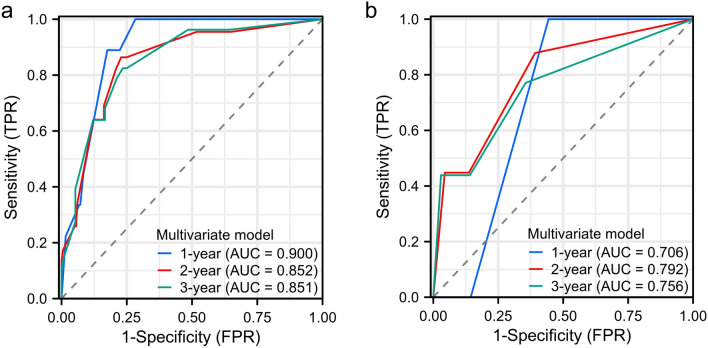
To investigate the prognostic value of lymph node status in patients with cervical cancer (CC) patients who underwent neoadjuvant chemotherapy (NACT) and followed hysterectomy. Patients in two referral centers were retrospectively analyzed. The baseline tumor size and radiological lymph node status (LNr) were evaluated on pre-NACT MRI. Tumor histology, differentiation and pathological lymph node status (LNp) were obtained from post-operative specimen. The log-rank test was used to compare survival between patient groups. Cox proportional hazards regression models were employed to estimate the hazard ratio (HR) of various factors with progression-free survival (PFS) and overall survival (OS). A total of 266 patients were included. Patients with 2018 FIGO IIIC showed worse PFS compared to those with FIGO IB-IIB (p < 0.001). The response rate in patients with LNp(-) was 64.1% (134/209), significantly higher than that of 45.6% (26/57) in patients with LNp( +) (p = 0.011). Multivariate Cox analysis identified the main independent predictors of PFS as LNp( +) (HR = 3.777; 95% CI 1.715-8.319), non-SCC (HR = 2.956; 95% CI 1.297-6.736), poor differentiation (HR = 2.370; 95% CI 1.130-4.970) and adjuvant radiation (HR = 3.266; 95% CI 1.183-9.019). The interaction between LNr and LNp regarding PFS were significant both for univariate and multivariate (P = 0.000171 and 1.5357e-7 respectively). In patients with LNr( +), a significant difference in PFS was observed between patients with LNp(-) and LNp( +) (p = 0.0027). CC patients with FIGO 2018 stage IIIC who underwent NACT and followed hysterectomy had worse PFS compared to those with IB-IIB. LNp( +), non-SCC, poor differentiation and adjuvant radiation were independent risk factors for PFS. The adverse prognostic value of LNp( +) was more significant in patients with LNr( +).
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures


Similar articles
-
The prognostic value of lymph node ratio in stage IIIC cervical cancer patients triaged to primary treatment by radical hysterectomy with systematic pelvic and para-aortic lymphadenectomy.J Gynecol Oncol. 2020 Jan;31(1):e1. doi: 10.3802/jgo.2020.31.e1. Epub 2019 Jun 24. J Gynecol Oncol. 2020. PMID: 31788991 Free PMC article.
-
[Effects of pre-chemotherapy hemoglobin and platelet levels in patients with stage Ib2-IIb cervical cancer treated with neoadjuvant chemotherapy followed by radical hysterectomy].Zhonghua Fu Chan Ke Za Zhi. 2012 Aug;47(8):577-81. Zhonghua Fu Chan Ke Za Zhi. 2012. PMID: 23141176 Chinese.
-
Lymph Node Ratio Is a Strong Prognostic Factor in Patients with Early-Stage Cervical Cancer Undergoing Minimally Invasive Radical Hysterectomy.Yonsei Med J. 2021 Mar;62(3):231-239. doi: 10.3349/ymj.2021.62.3.231. Yonsei Med J. 2021. PMID: 33635013 Free PMC article.
-
[Prognostic analysis of stage Ⅰb2 andⅡa2 cervical squamous cancer without high risk factors treated with neo-adjuvant chemotherapy and radical hysterectomy].Zhonghua Fu Chan Ke Za Zhi. 2018 Apr 25;53(4):248-256. doi: 10.3760/cma.j.issn.0529-567x.2018.04.008. Zhonghua Fu Chan Ke Za Zhi. 2018. PMID: 29747270 Chinese.
-
The efficacy of neoadjuvant chemotherapy in different histological types of cervical cancer.Gynecol Oncol. 2014 Aug;134(2):419-25. doi: 10.1016/j.ygyno.2014.06.001. Epub 2014 Jun 8. Gynecol Oncol. 2014. PMID: 24918866 Review.
Cited by
-
Computed tomography-based radiomics modeling to predict patient overall survival in cervical cancer with intensity-modulated radiotherapy combined with concurrent chemotherapy.J Int Med Res. 2025 Mar;53(3):3000605251325996. doi: 10.1177/03000605251325996. Epub 2025 Mar 22. J Int Med Res. 2025. PMID: 40119689 Free PMC article.
-
Establishment of a Novel Risk Stratification System Integrating Clinical and Pathological Parameters for Prognostication and Clinical Decision-Making in Early-Stage Cervical Cancer.Cancer Med. 2024 Nov;13(22):e70394. doi: 10.1002/cam4.70394. Cancer Med. 2024. PMID: 39555813 Free PMC article.
-
Preparation of Electrochemical Sensors Based on Graphene/Ionic Liquids and the Quantitative Detection and Toxicity Evaluation of Tetracycline.Nanomaterials (Basel). 2025 Feb 10;15(4):263. doi: 10.3390/nano15040263. Nanomaterials (Basel). 2025. PMID: 39997826 Free PMC article.
References
-
- NCCN Guidelines for Patients: Cervical Cancer. Cerv. Cancer (2022).
