

Endometriosis MR mimickers: T2-hypointense lesions
- PMID: 38267633
- PMCID: PMC10808434
- DOI: 10.1186/s13244-023-01588-2
Endometriosis MR mimickers: T2-hypointense lesions
Erratum in
-
Correction: Endometriosis MR mimickers: T2-hypointense lesions.Insights Imaging. 2024 Mar 25;15(1):89. doi: 10.1186/s13244-024-01674-z. Insights Imaging. 2024. PMID: 38526611 Free PMC article. No abstract available.
Abstract
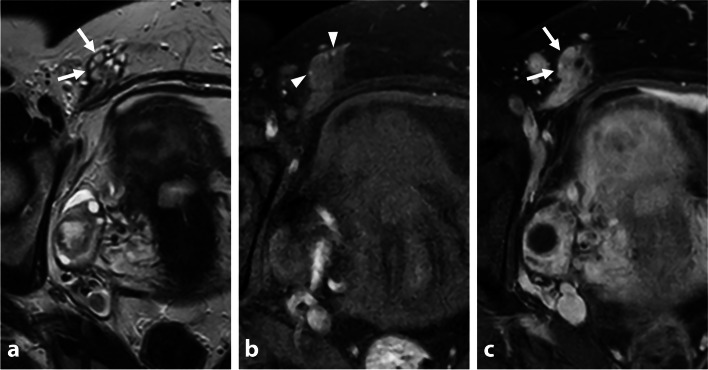
Endometriosis is a common crippling disease in women of reproductive age. Magnetic resonance imaging (MRI) is considered the cornerstone radiological technique for both the diagnosis and management of endometriosis. While its sensitivity, especially in deep infiltrating endometriosis, is superior to that of ultrasonography, many sources of false-positive results exist, leading to a lack of specificity. Hypointense lesions or pseudo-lesions on T2-weighted images include anatomical variants, fibrous connective tissues, benign and malignant tumors, feces, surgical materials, and post treatment scars which may mimic deep pelvic infiltrating endometriosis. False positives can have a major impact on patient management, from diagnosis to medical or surgical treatment. This educational review aims to help the radiologist acknowledge MRI criteria, pitfalls, and the differential diagnosis of deep pelvic infiltrating endometriosis to reduce false-positive results. Critical relevance statement MRI in deep infiltrating endometriosis has a 23% false-positive rate, leading to misdiagnosis. T2-hypointense lesions primarily result from anatomical variations, fibrous connective tissue, benign and malignant tumors, feces, surgical material, and post-treatment scars. Key points • MRI in DIE has a 23% false-positive rate, leading to potential misdiagnosis.• Anatomical variations, fibrous connective tissues, neoplasms, and surgical alterations are the main sources of T2-hypointense mimickers.• Multisequence interpretation, morphologic assessment, and precise anatomic localization are crucial to prevent overdiagnosis.• Gadolinium injection is beneficial for assessing endometriosis differential diagnosis only in specific conditions.
Keywords: Deep infiltrating endometriosis; Endometriosis; Genital diseases; Magnetic resonance imaging; Pelvic inflammatory disease.
© 2024. The Author(s).
Conflict of interest statement
Pascal Rousset reported consultant fees from Ziwig and EDAP TMS France and reported receiving lecture fees from Bracco and compensation for serving on the board from Guerbet.
Stéphanie Nougaret is funded by the European Research Grant (ERC starting grant) and Integrated Cancer Research Grant (SIRIC).
Isabelle Thomassin-Naggara reported receiving lecture fees from General Electric, Siemens, Canon, and GSK; lecture fees and compensation for serving on the board from Guerbet; compensation for serving on the board from Bayer; lecture fees from Incepto, ICAD, Fujifilm, and Hologic; and lecture fees and compensation for serving on the board from Bracco.
Figures











References
-
- (2012) Endometriosis and infertility: a committee opinion. Fertil Steril 98:591–598. 10.1016/j.fertnstert.2012.05.031 - PubMed
Publication types
LinkOut - more resources
Full Text Sources
