

Occult metastasis is no burden factor in oral squamous cell carcinoma patients when adhering to a standardized approach in neck dissection
- PMID: 38267767
- PMCID: PMC10808318
- DOI: 10.1007/s00784-024-05514-8
Occult metastasis is no burden factor in oral squamous cell carcinoma patients when adhering to a standardized approach in neck dissection
Abstract
Objectives: Management of the neck in patients with oral squamous cell carcinoma (OSCC) is pivotal to oncologic control and survival. However, there is controversy regarding necessity of neck dissection (ND) in patients with clinically node-negative neck. We aimed to assess risk factors for occult metastasis and to explore whether the presence of occult lymph node metastases (LNMs) has an impact on recurrence and survival.
Material and methods: A retrospective cohort study was performed including patients with primary OSCC who underwent radical tumor resection and ND in a high-volume center adhering to the prevailing German guideline. The ND was performed according to a standardized approach.
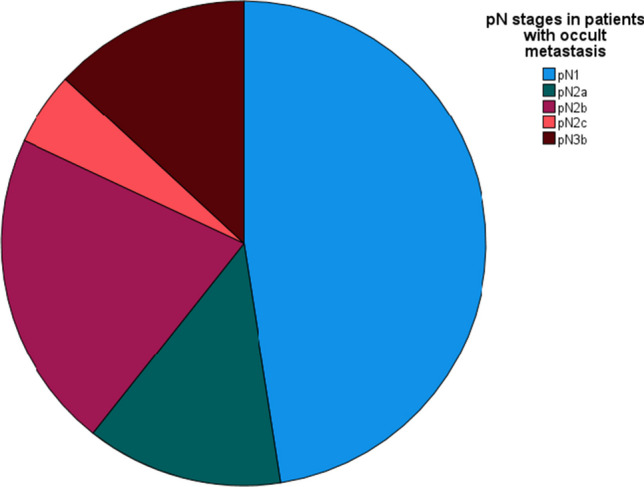
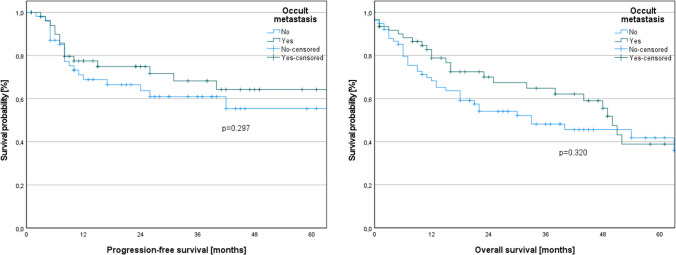
Results: Four hundred twenty-one patients with primary surgically treated OSCC were included. The incidence of occult metastasis was 14.49%. A pathological T stage > 1 (multivariate analysis, odds ratio (OR) 3.958, p = 0.042) and the presence of extranodal extension in LNMs (multivariate analysis, OR 0.287, p = 0.020) were identified as independent risk factors for occult metastasis. When comparing patients with and without occult metastasis, there were no significant differences in terms of progression-free survival (log-rank, p = 0.297) and overall survival (log-rank, p = 0.320). There were no cases of ipsilateral neck recurrence. One patient developed contralateral neck metastasis; however, he initially presented with a unilateral pT1 pN0 tumor.
Conclusions: Overall, our findings suggest that conducting a standardized approach in ND should be applied in terms of management of the neck in order to maintain survival rates and to prevent neck recurrence in OSCC patients.
Clinical relevance: None of the risk factors for occult metastasis can be reliably assessed preoperatively. Although elective ND does not guarantee the complete prevention of neck recurrence, it increases the likelihood of either timely removal of micrometastases or strengthens the justification for adjuvant therapy. Consequently, this approach leads to improvements in clinical outcomes.
Keywords: Lymph node metastasis; Neck dissection; Occult metastasis; Oral squamous cell carcinoma.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
The authors have no financial or non-financial conflicts of interest to disclose.
Figures

References
-
- Moratin J, Horn D, Metzger K, Ristow O, Flechtenmacher C, Engel M, Hoffmann J, Freier K, Freudlsperger C. Squamous cell carcinoma of the mandible - patterns of metastasis and disease recurrence in dependence of localization and therapy. J Craniomaxillofac Surg. 2020;48:1158–1163. doi: 10.1016/j.jcms.2020.10.006. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
