

The impact of obesity on different glucose tolerance status with incident cardiovascular disease and mortality events over 15 years of follow-up: a pooled cohort analysis
- PMID: 38267963
- PMCID: PMC10809520
- DOI: 10.1186/s13098-023-01253-0
The impact of obesity on different glucose tolerance status with incident cardiovascular disease and mortality events over 15 years of follow-up: a pooled cohort analysis
Abstract
Background: The effect of obesity in different glucose tolerance statuses i.e. normoglycemia (NGT), pre-diabetes, and type 2 diabetes (T2DM) on cardiovascular disease (CVD) and mortality has been an area of ongoing debate and uncertainty. In the present study, we aimed to examine the impact of being obese, whether general or central separately, in comparison with non-obese in different glucose tolerance statuses on the above outcomes.
Methods: The study population included 18,184 participants aged 30-60 years (9927 women) from three longitudinal studies, including Atherosclerosis Risk in Communities, Multi-Ethnic Study of Atherosclerosis, and Tehran Lipid and Glucose Study. Glucose tolerance status was defined as NGT (fasting plasma glucose < 5.55 mmol/L), pre-diabetes (5.55-7.00 mmol/L), and T2DM (≥ 7 mmol/L or taking any medication for diabetes). Moreover, general and central obesity were defined based on body mass index and waist circumference (WC), respectively. Multivariable stratified Cox regression analysis was used to estimate hazard ratios (HRs (95% CI)) for CVD and mortality events.
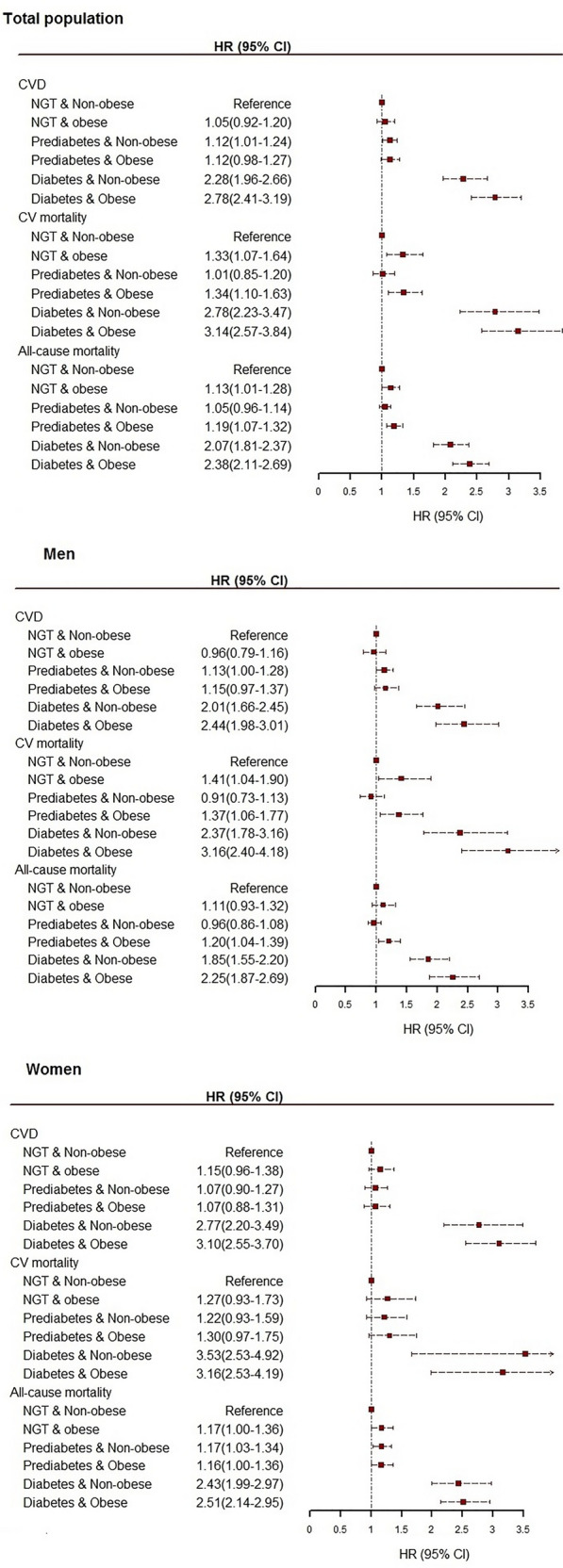
Results: During a 16-year follow-up, 2733 CVD events, 1101 CV mortality, and 3678 all-cause mortality events were recorded. We observed that being generally obese in comparison with non-obese increased the risk of CV and all-cause mortality in all glucose tolerance statuses; while considering CVD events, only among individuals with T2DM, the presence of general obesity was associated with marginally significant higher risk [1.19 (0.98-1.43); p-value = 0.07]. Regarding central adiposity, multivariate analysis revealed that elevated WC in NGT participants is associated with incident CVD [1.27(1.12-1.46)] and all-cause mortality [1.13(1.00-1.28)]. Moreover, central adiposity increased the risk of CV mortality in pre-diabetes individuals [1.47 (1.11-1.95)].
Conclusion: Findings from this pooled prospective cohort studies provide evidence that general obesity shows an unfavorable association with CV and all-cause mortality among the general population irrespective of their glucose tolerance statusThe findings imply that it's important to take into account the requirement and magnitude of weight reduction in people who are obese when offering guidance.
Keywords: Cardiovascular disease; Glucose intolerance status; Mortality; Obesity.
© 2024. The Author(s).
Conflict of interest statement
None declared.
Figures
Similar articles
-
Changes in Fasting plasma glucose status and risk of mortality events in individuals without diabetes over two decades of Follow-up: a pooled cohort analysis.Cardiovasc Diabetol. 2022 Dec 3;21(1):267. doi: 10.1186/s12933-022-01709-z. Cardiovasc Diabetol. 2022. PMID: 36463152 Free PMC article.
-
Change in glucose intolerance status and risk of incident cardiovascular disease: Tehran Lipid and Glucose Study.Cardiovasc Diabetol. 2020 Mar 30;19(1):41. doi: 10.1186/s12933-020-01017-4. Cardiovasc Diabetol. 2020. PMID: 32228577 Free PMC article.
-
Impact of diabesity phenotype on cardiovascular diseases, major cardiovascular events and all-cause mortality.Sci Rep. 2023 Jul 12;13(1):11266. doi: 10.1038/s41598-023-38221-7. Sci Rep. 2023. PMID: 37438573 Free PMC article.
-
Development of type 2 diabetes mellitus in people with intermediate hyperglycaemia.Cochrane Database Syst Rev. 2018 Oct 29;10(10):CD012661. doi: 10.1002/14651858.CD012661.pub2. Cochrane Database Syst Rev. 2018. PMID: 30371961 Free PMC article.
-
Nordic dietary patterns and cardiometabolic outcomes: a systematic review and meta-analysis of prospective cohort studies and randomised controlled trials.Diabetologia. 2022 Dec;65(12):2011-2031. doi: 10.1007/s00125-022-05760-z. Epub 2022 Aug 26. Diabetologia. 2022. PMID: 36008559 Free PMC article.
Cited by
-
The modified role including mediating and synergistic interactive effects of glucose tolerance status in the associations between relative fat mass and the risks of cardiovascular disease and all-cause mortality from the 4C cohort study.Diabetol Metab Syndr. 2024 Dec 26;16(1):313. doi: 10.1186/s13098-024-01558-8. Diabetol Metab Syndr. 2024. PMID: 39726036 Free PMC article.
References
-
- WHO . The top 10 causes of death. Geneva: World Health Organization; 2018.
-
- IDF Diabetes Atlas 2021 – 10th edn. https://diabetesatlas.org/idfawp/resource-files/2021/07/IDF_Atlas_10th_E.... - PubMed
LinkOut - more resources
Full Text Sources
