

[Current Features and Mortality Risk Factors in Cardiogenic Shock due to Myocardial Infarction in a Latin-American hospital]
- PMID: 38268514
- PMCID: PMC10804818
- DOI: 10.47487/apcyccv.v1i4.89
[Current Features and Mortality Risk Factors in Cardiogenic Shock due to Myocardial Infarction in a Latin-American hospital]
Abstract
Objective: To know the clinical characteristics and determine the related factors to higher in-hospital mortality in patients with cardiogenic shock (CS) due to myocardial infarction in a Peruvian reference hospital.
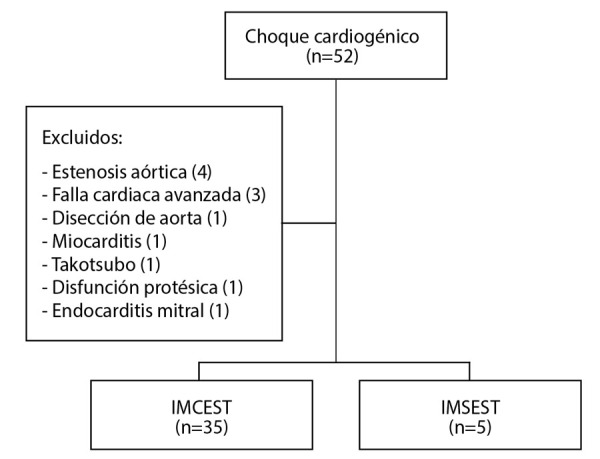
Materials and methods: . We conducted a prospective single-center cohort study, to evaluate the clinical characteristics, treatment, and complications of patients with CS due to myocardial infarction from March 2019 to August 2020 at the Instituto Nacional Cardiovascular INCOR. Factors related to higher in-hospital mortality and during follow-up were evaluated. Also, the IABP shock II score was applied to stratify the cohort.
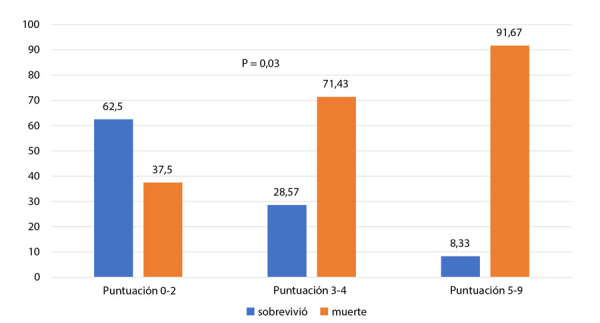
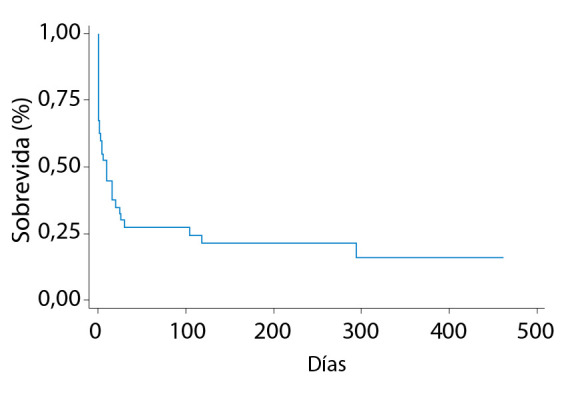
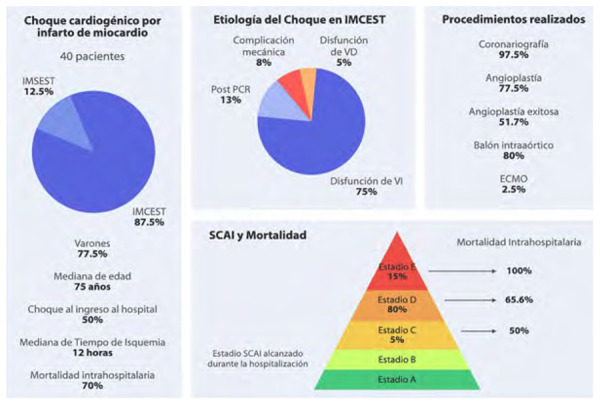
Results: Forty patients were included in the study, 75% of cases were due to left ventricular dysfunction, most of the men and with a median age of 75 (69-82) years. Fifty percent of cases presented CS after admission to the emergency room. Patients stratified by the IABP shock II score as low, intermediate, and high risk, had in-hospital mortality of 37.5%, 71.4%, and 91.6% respectively. In a hospital, mortality was 70%, higher in women, in those over 75 years old, and in those who developed CS during their hospitalization. Serum lactate > 4 mmol/L in univariate analysis was associated with higher mortality risk (HR: 2.8; IC:1.6-3.6, p=0.009). Survival to the end of the study was 12.8%.
Conclusions: CS due to myocardial infarction is a clinical entity with high mortality in spite of revascularization and the available treatment in our reality. The highest mortality predictor was the serum lactate at admission > 4 mmol/L. The IABP shock II score showed to be an accurate parameter to stratify the death risk in our population.
Objetivo.: Conocer las características clínicas y determinar los factores relacionados a mayor mortalidad en pacientes con choque cardiogénico (CC) por infarto de miocardio en un hospital de referencia peruano.
Materiales y métodos.: Cohorte única prospectiva donde se evaluó la presentación, tratamiento y complicaciones de pacientes con CC por infarto de miocardio atendidos entre marzo 2019 a agosto 2020 en el Instituto Nacional Cardiovascular - INCOR. Se evaluaron los factores relacionados con mayor mortalidad hospitalaria y en el seguimiento, además del uso del score IABP shock II en la población de estudio.
Resultados.: Cuarenta pacientes fueron incluidos, el 75% con CC por disfunción ventricular izquierda, la mayoría varones con edad de 75 (69-82) años. Un 50% de casos presentaron CC luego del ingreso a emergencia. Los pacientes estratificados mediante el score IABP shock II como bajo, intermedio y alto riesgo, tuvieron una mortalidad intrahospitalaria de 37,5; 71;4 y 91,6% respectivamente. La mortalidad intrahospitalaria fue 70%, mayor en mujeres, mayores de 75 años y en los que desarrollaron el CC durante la hospitalización. En el análisis univariado, el lactato sérico > 4 mmol/L al ingreso se relacionó con mayor mortalidad (HR:2,8; IC:1,6-3,6, p=0,009). La sobrevida hasta el término del estudio fue de 12,8%.
Conclusiones.: EL CC por infarto de miocardio representa una entidad clínica de elevada mortalidad a pesar de la revascularización y el tratamiento disponible en nuestra realidad. El mayor predictor de mortalidad fue el valor de lactato sérico mayor a 4 mmol/L al ingreso. El score IABP shock II demostró ser un buen parámetro para estratificar el riesgo de muerte en nuestra población.
Keywords: Cardiogenic Shock; Mortality; Myocardial Infarction; Peru.
Conflict of interest statement
Conflictos de interés: Los autores no presentan conflictos de interés.
Figures
References
-
- Zeymer U, Bueno H, Granger CB, Hochman J, Huber K, Lettino M, et al. Acute Cardiovascular Care Association position statement for the diagnosis and treatment of patients with acute myocardial infarction complicated by cardiogenic shock A document of the Acute Cardiovascular Care Association of the European Society of Cardiology. Eur Heart J Acute Cardiovasc Care. 2020;9(2):183–197. doi: 10.1177/204887261989425. - DOI - PubMed
-
- Aissaoui N, Puymirat E, Tabone X, Charbonnier B, Schiele Fr, Lefèvre T, et al. Improved outcome of cardiogenic shock at the acute stage of myocardial infarction A report from the USIK 1995, USIC 2000, and FAST-MI French Nationwide Registries. Eur Heart J. 2012;33(20):2535–2543. - PubMed
-
- Poss J, Köster J, Fuernau G, Eitel I, De Waha S, Ouarrak T, et al. Risk Stratification for Patients in Cardiogenic Shock After Acute Myocardial Infarction. J Am Coll Cardiol. 2017;69(15):1913–1920. - PubMed
-
- Chacón-Diaz M, Vega A, Aráoz O, Ríos P, Baltodano R, Villanueva F, et al. Epidemiological characteristics of ST-segment elevation myocardial infarction in Peru Results of the peruvian registry of ST-segment elevation myocardial infarction (PERSTEMI) Arch Cardiol Mex. 2018;88(5):403–412. - PubMed
-
- Chacón-Diaz M, Araoz-Tarco O, Alarco-León W, Aguirre-Zurita O, Rosales-Vidal M, Rebaza-Miyasato P. Heart failure complicating myocardial infarction A report of the peruvian registry of ST-elevation myocardial infarction (PERSTEMI) Arch Cardiol Mex. 2018;88(5):447–453. - PubMed
Publication types
LinkOut - more resources
Full Text Sources