

Exploring the risk of infection events in patients with asthma receiving anti-IL-5 monoclonal antibodies: A rapid systematic review and a meta-analysis
- PMID: 38268596
- PMCID: PMC10805771
- DOI: 10.1016/j.heliyon.2023.e23725
Exploring the risk of infection events in patients with asthma receiving anti-IL-5 monoclonal antibodies: A rapid systematic review and a meta-analysis
Abstract
Introduction: Benralizumab, mepolizumab, and reslizumab are novel monoclonal antibodies approved for asthma, targeting eosinophilic inflammation. Benralizumab is directed against IL-5 receptor (IL-5R), while mepolizumab and reslizumab are directed against IL-5. The three drugs cause a reduction in eosinophils, but benralizumab also causes a cytotoxic effect on eosinophils and basophils. Recently, it has been reported that suboptimal responders to benralizumab presented exacerbations associated with concomitant infections and sputum neutrophilia and the incidence of infections was greater in patients receiving benralizumab compared to mepolizumab and reslizumab. For this reason, we wanted to explore potential differences in terms of infectious adverse events between the three different anti-IL-5 antibodies.
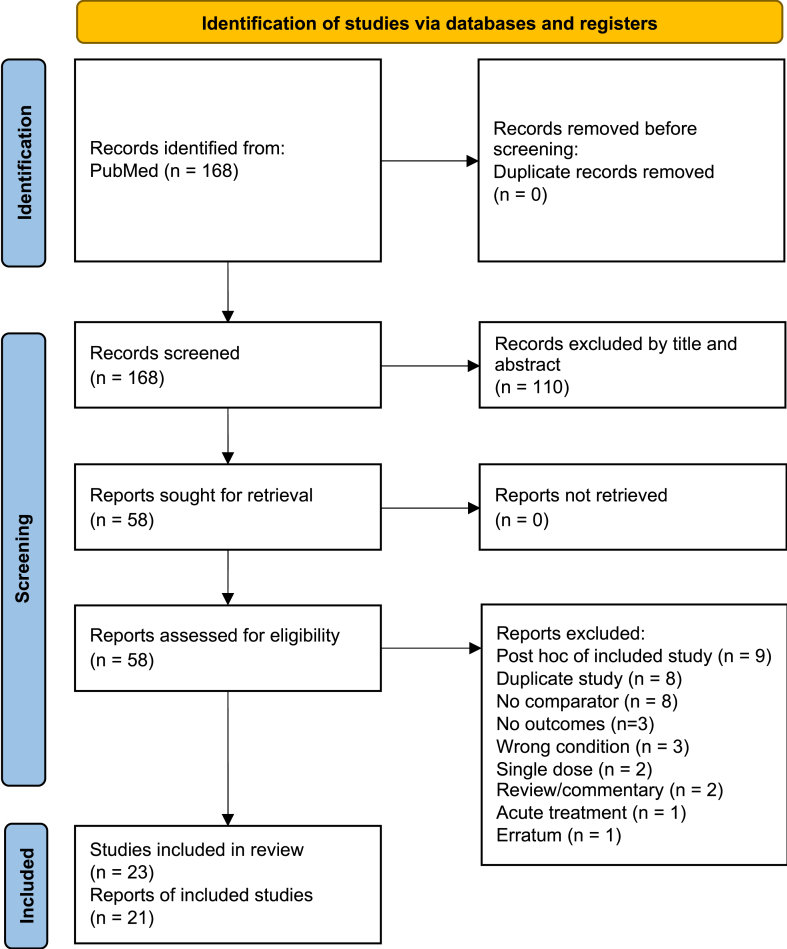
Methods: We performed a rapid systematic review on PubMed up to April 28, 2022. We included randomized controlled trials (RCTs) evaluating benralizumab, mepolizumab, or reslizumab in patients with asthma. Included outcomes were the reporting of any respiratory tract infection and any emergency department (ED) or hospital admission for infection or asthma exacerbation. A Mantel-Haenszel meta-analysis was performed with Cochrane RevMan 5.4 to estimate pooled odds ratios (OR) with 95 % confidence intervals (CI). A subgroup analysis for the different active treatments was performed.
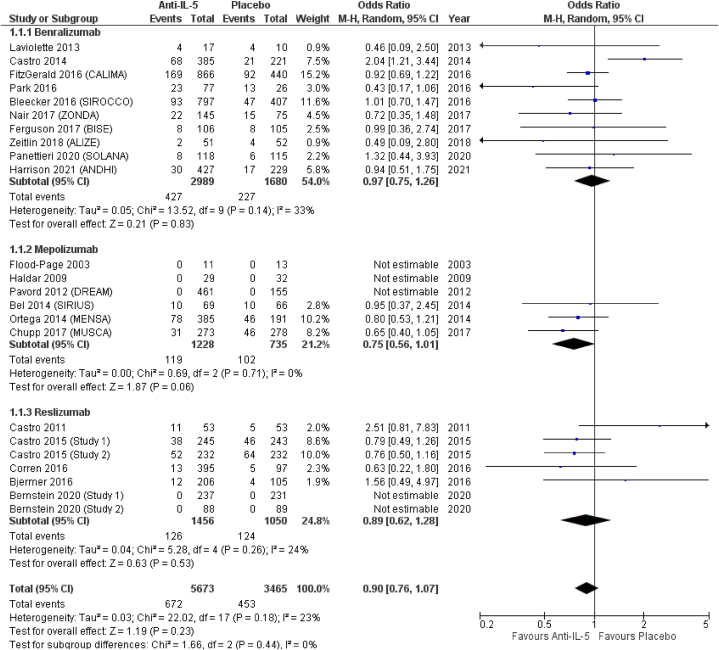
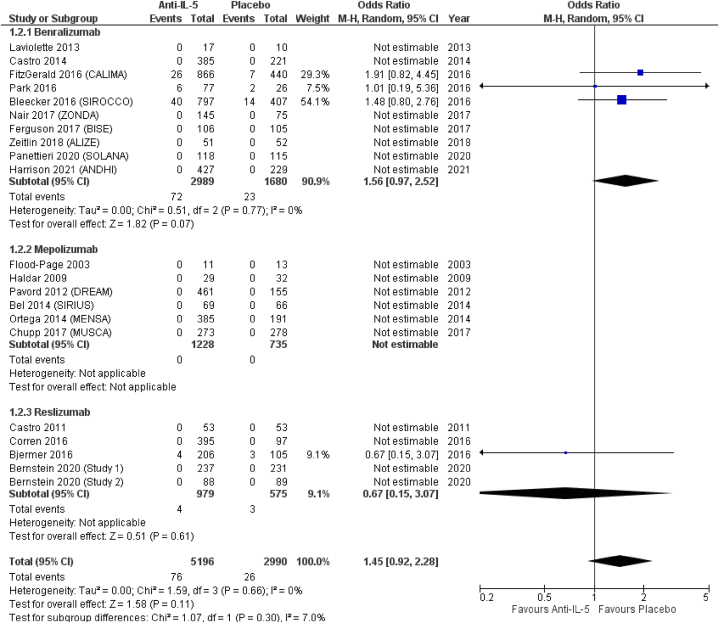
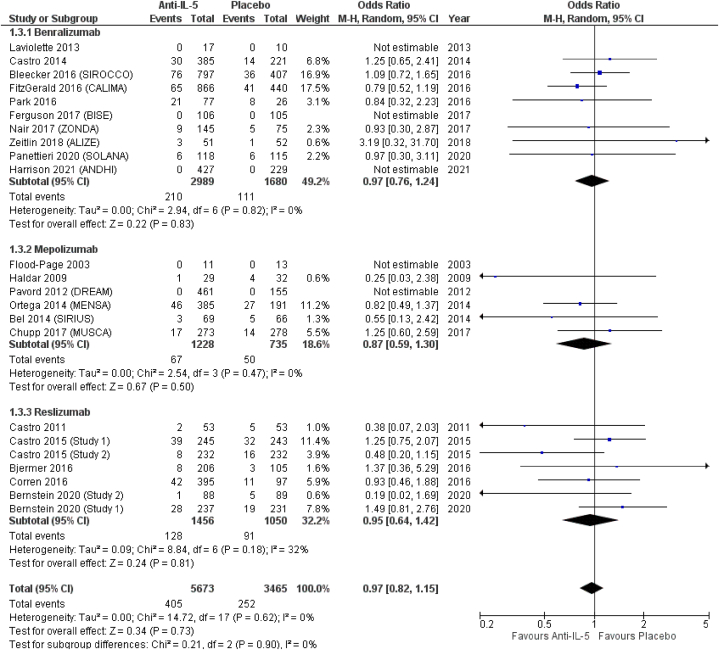
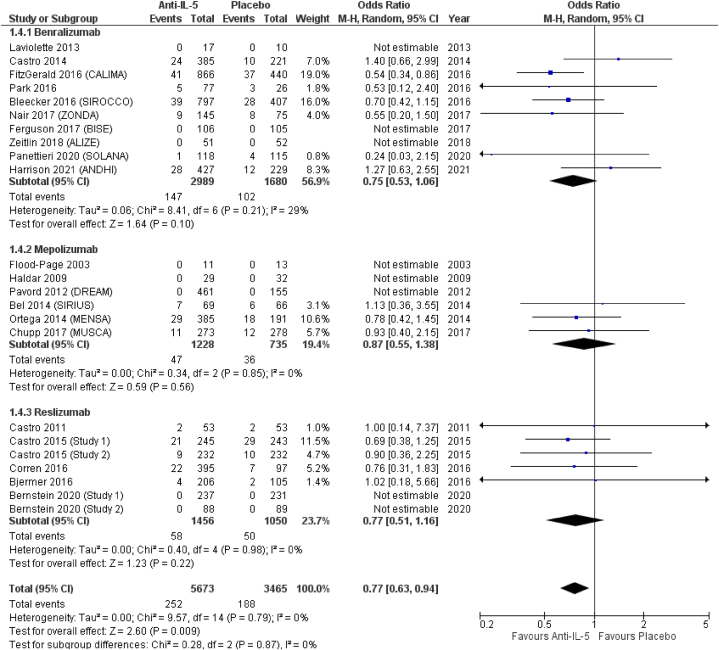
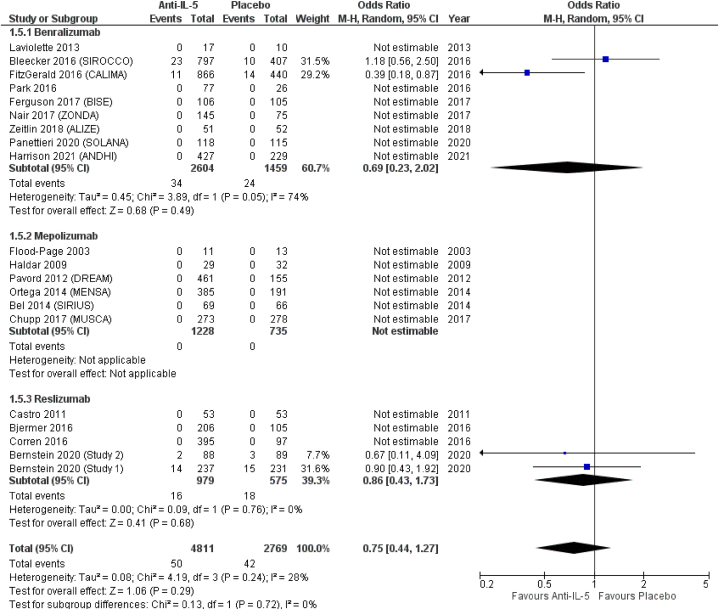
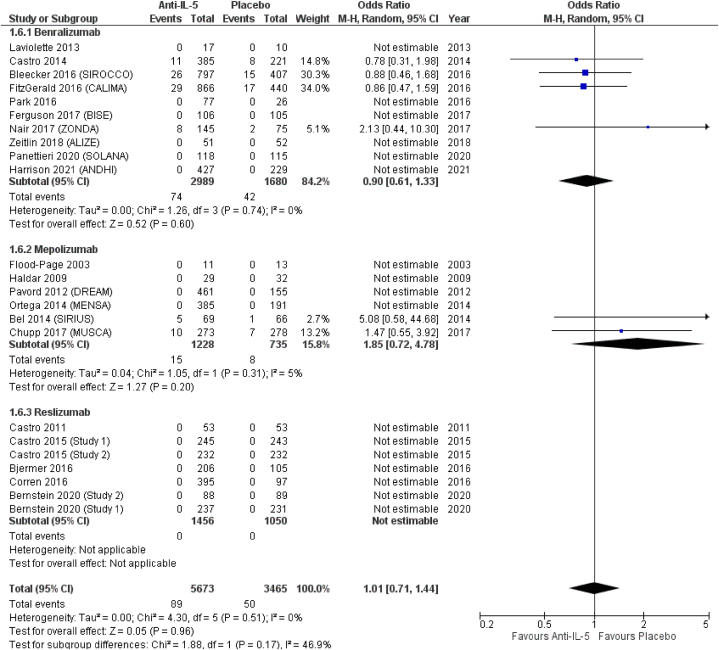
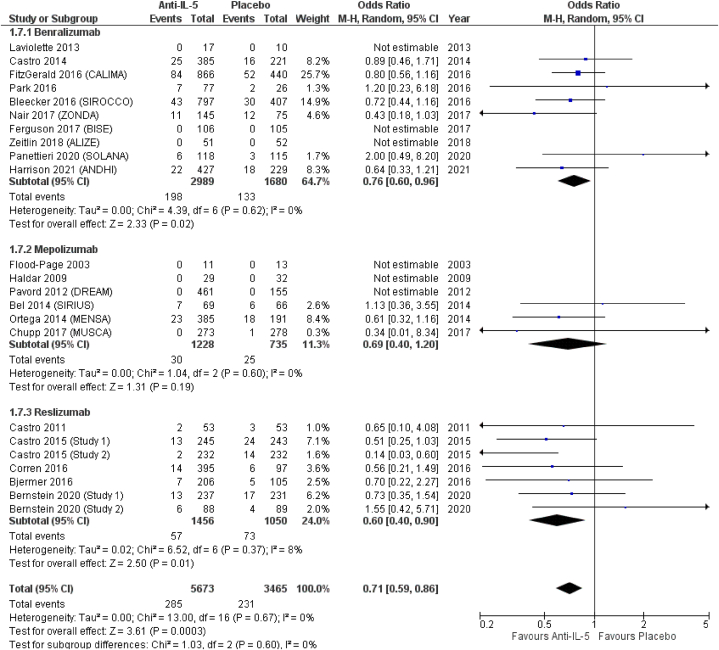
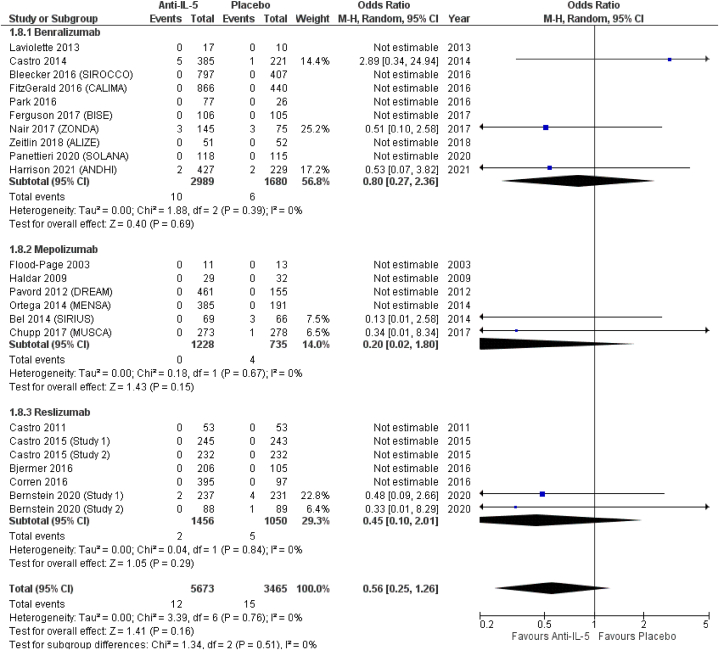
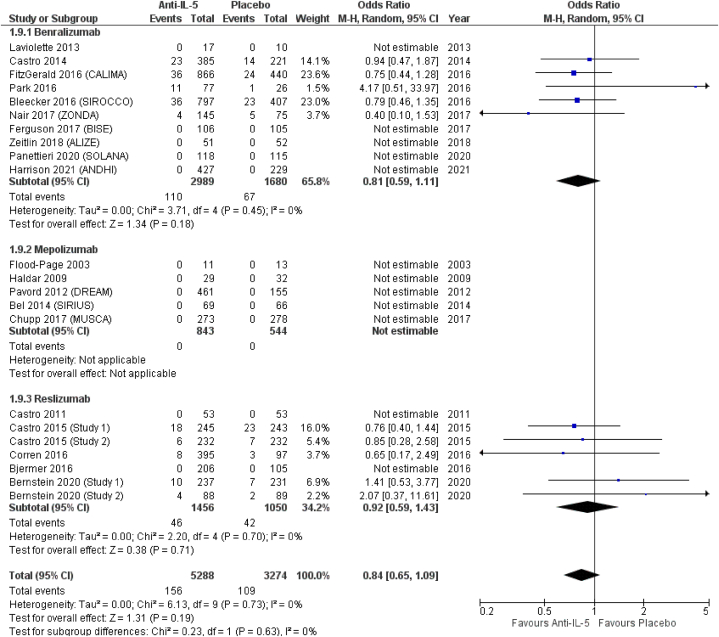
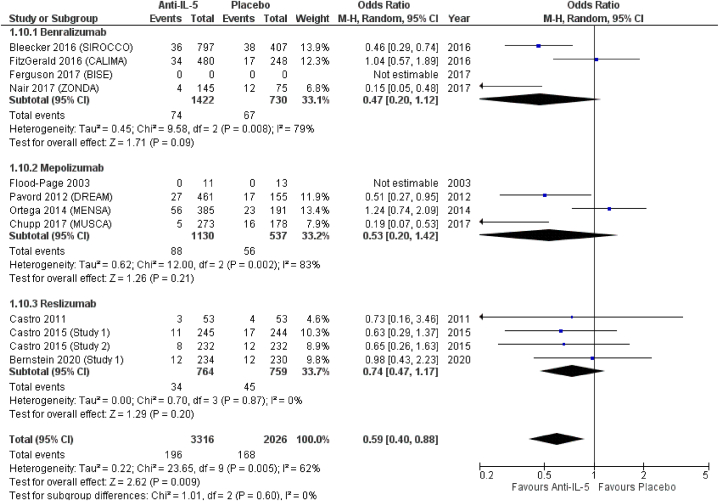
Results: From 163 references we included 21 studies reporting the results of 23 different RCTs for a total population of 9156 patients. All studies compared anti-IL-5 antibodies against placebo. Anti-IL-5 treatment resulted in non-significant differences compared to placebo in the odds for nasopharyngitis (OR = 0.90; 95 % CI from 0.76 to 1.07), pharyngitis (OR = 1.45; 95 % CI from 0.92 to 2.28), upper respiratory tract infection (URTI) (OR = 0.97; 95 % CI from 0.82 to 1.15), rhinitis (OR = 1.01; 95 % CI from 0.71 to 1.44), pneumonia (OR = 0.56; 95 % CI from 0.10 to 2.01), and influenza (OR = 0.84; 95 % CI from 0.65 to 1.09). We observed significant reductions in the reporting of sinusitis (OR = 0.75; 95 % CI from 0.53 to 1.06), bronchitis (OR = 0.71; 95 % CI from 0.59 to 0.86), and ED or hospital admission due to asthma exacerbation for overall anti-IL-5 antibodies compared to placebo (OR = 0.59; 95 % CI from 0.40 to 0.88). We were not able to discriminate whether exacerbations were associated with infections or to increased sputum eosinophilia. From the subgroup analysis, we observed differences in directions and magnitudes of the effect size in the reporting of some events. Benralizumab was associated with increased odds of pharyngitis (OR = 1.56; 95 % CI from 0.97 to 2.52) and a similar trend was observed for mepolizumab in the reporting of rhinitis (OR = 1.85; 95 % CI from 0.72 to 4.78), both non-statistically significant. In terms of effect size, benralizumab also showed higher odds for bronchitis and pneumonia in comparison to mepolizumab and reslizumab (OR = 0.76, OR = 0.69, and OR = 0.60 for bronchitis and OR = 0.80, OR = 0.20, and OR = 0.45, respectively, all non-significant).
Conclusion: Anti-IL-5 treatments might have different effects on the reporting of some infection events in patients with asthma. However, the evidence is limited by sample size and far than conclusive and suggest the need of future studies to evaluate the risk of infections in patients with asthma receiving anti-IL-5 treatments.
Keywords: Benralizumab; IL-5; Infection; Mepolizumab; Meta-analysis; Reslizumab.
© 2023 The Authors.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
References
-
- King G.G., James A., Harkness L., Wark P.A.B. Pathophysiology of severe asthma: we’ve only just started. Respirology. Australia. 2018;23:262–271. - PubMed
-
- Heaney L.G., Perez de Llano L., Al-Ahmad M., Backer V., Busby J., Canonica G.W., et al. Eosinophilic and noneosinophilic asthma: an expert consensus framework to characterize phenotypes in a global real-life severe asthma cohort. Chest. United States. 2021;160:814–830. - PubMed
-
- Gieseck R.L., 3rd, Wilson M.S., Wynn T.A. Type 2 immunity in tissue repair and fibrosis. Nat Rev Immunol. England. 2018;18:62–76. - PubMed
-
- Harley W.B., Blaser M.J. Disseminated coccidioidomycosis associated with extreme eosinophilia. Clin Infect Dis an Off Publ Infect Dis Soc Am. United States. 1994;18:627–629. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
