

Can Unilateral Therapeutic Central Lymph Node Dissection Be Performed in Papillary Thyroid Cancer with Lateral Neck Metastasis?
- PMID: 38268664
- PMCID: PMC10805041
- DOI: 10.14744/SEMB.2023.22309
Can Unilateral Therapeutic Central Lymph Node Dissection Be Performed in Papillary Thyroid Cancer with Lateral Neck Metastasis?
Abstract
Objectives: Unilateral or bilateral prophylactic central neck dissection (CND) in papillary thyroid cancer (PTC) is still controversial. We aimed to evaluate the risk factors for contralateral paratracheal lymph node metastasis and whether CND might be performed unilaterally.
Methods: Prospectively collected data of patients who underwent bilateral CND and lateral neck dissection (LND) with thyroidectomy due to PTC with lateral metastases, between January 2012 and November 2019, were evaluated retrospectively. The patients were divided into two groups according to the presence (Group 1) and absence (Group 2) of metastasis in the contralateral paratracheal region.A total of 42 patients (46 ±15.7 years) were operated. In the contralateral paratracheal region, Group 1 (35.7%) had metastases, while Group 2 (64.3%) had no metastases. In groups 1 and 2, metastasis rates were 100% vs 77.8% (p=0.073), 46.7% vs 18.5% (p=0.078), and 80% vs 40.7% (p=0.023) for the ipsilateralparatracheal, prelaryngeal and pretracheal lymph nodes, respectively.The number of metastatic lymph nodes in the central region was significantly higher in Group 1 compared to Group 2 as; 10.7±8.4 vs. 2.6±2.4 (p=0.001) in bilateral central region material; 8.3±7.4 vs. 2.9±2.7 (p=0.001) in lateral metastasis with ipsilateral unilateral central region; 3.8±3.4 vs. 1.9±1.9 (p=0.023) in ipsilateralparatracheal area; and 3.7±4.6 vs. 0.6±0.9 (p=0.001) in pretracheal region, respectively. However, no significant difference was found regarding the prelaryngeal region material (0.9±1.8 vs. 0.2±0.4 (p=0.71)).
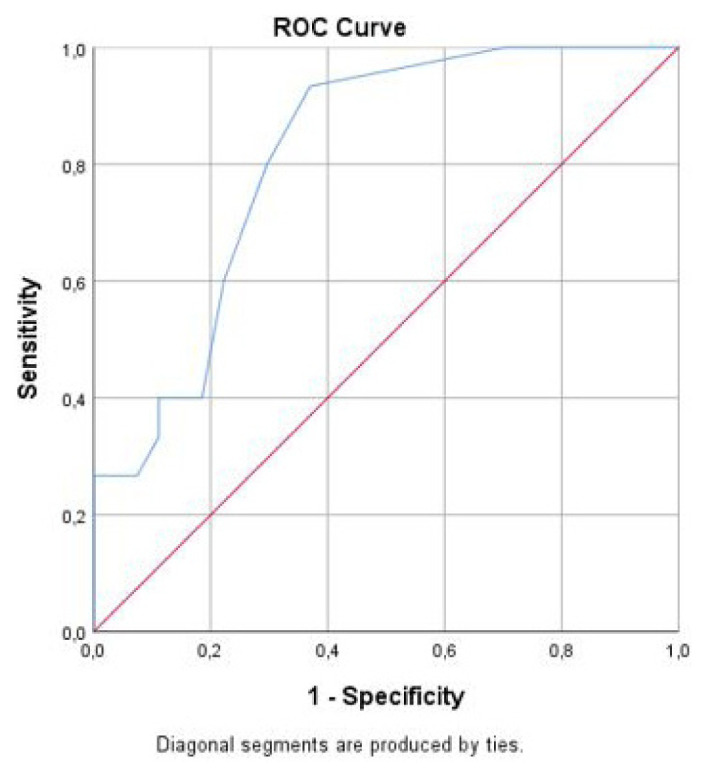
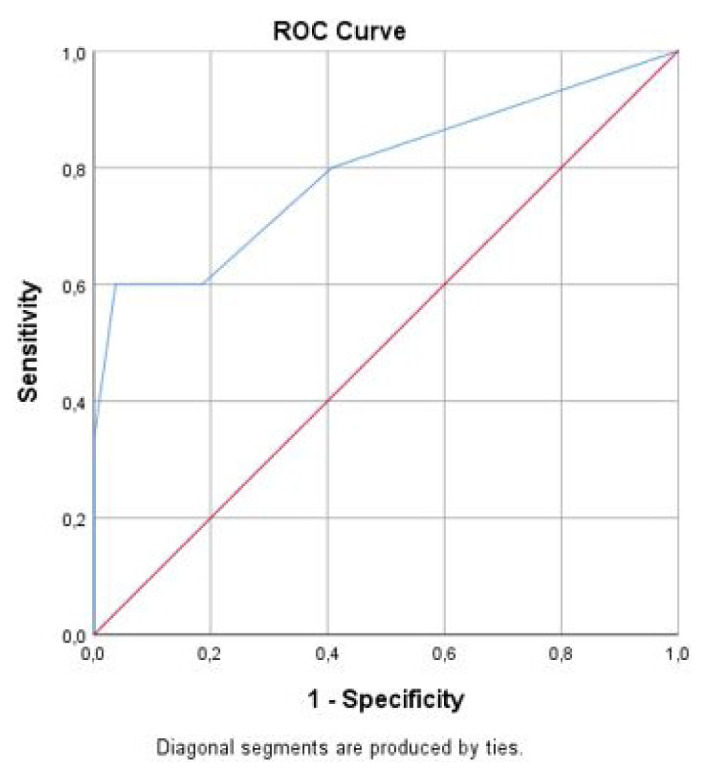
Results: >2 metastatic central lymph nodes in unilateral CND material (AUC: 0.814, p<0.001, J=0.563) can estimate contralateral paratracheal metastasis with 93% sensitivity, 63% specificity, while >2 pretracheal metastatic lymph nodes (AUC: 0.795, p<0.001, J: 0.563) can estimate contralateral paratracheal metastasis with 60% sensitivity and 96.3% specificity.
Conclusion: In patients with lateral metastases, the rate of ipsilateralparatracheal metastasis is 85%, while the rate of contralateral paratracheal metastasis is 35.7%. The number of ipsilateral central region or pretracheal lymph node metastases may be helpful in predicting contralateral paratracheal lymph node metastases. Notably, unilateral CND may be performed in the presence of ≤ 2 metastases in the ipsilateral central region.
Keywords: Central neck dissection; lateral neck metastasis; papillary thyroid cancer.
© Copyright 2023 by The Medical Bulletin of Sisli Etfal Hospital.
Conflict of interest statement
None declared.
Figures
Similar articles
-
Predictive factors of contralateral paratracheal lymph node metastasis in unilateral papillary thyroid carcinoma.Eur J Surg Oncol. 2015 Jun;41(6):746-50. doi: 10.1016/j.ejso.2015.02.013. Epub 2015 Apr 2. Eur J Surg Oncol. 2015. PMID: 25882035
-
Pretracheal Lymph Node Subdivision in Predicting Contralateral Central Lymph Node Metastasis for Unilateral Papillary Thyroid Carcinoma: Preliminary Results.Front Endocrinol (Lausanne). 2022 Jul 18;13:921845. doi: 10.3389/fendo.2022.921845. eCollection 2022. Front Endocrinol (Lausanne). 2022. PMID: 35923620 Free PMC article.
-
Predictive factors and pattern of central lymph node metastasis in unilateral papillary thyroid carcinoma.Auris Nasus Larynx. 2016 Feb;43(1):79-83. doi: 10.1016/j.anl.2015.09.005. Epub 2015 Oct 3. Auris Nasus Larynx. 2016. PMID: 26441368
-
Role and Extent of Neck Dissection for Neck Lymph Node Metastases in Differentiated Thyroid Cancers.Sisli Etfal Hastan Tip Bul. 2021 Dec 29;55(4):438-449. doi: 10.14744/SEMB.2021.76836. eCollection 2021. Sisli Etfal Hastan Tip Bul. 2021. PMID: 35317376 Free PMC article. Review.
-
Standards and Definitions in Neck Dissections of Differentiated Thyroid Cancer.Sisli Etfal Hastan Tip Bul. 2018 Oct 1;52(3):149-163. doi: 10.14744/SEMB.2018.14227. eCollection 2018. Sisli Etfal Hastan Tip Bul. 2018. PMID: 32595391 Free PMC article. Review.
References
-
- Haugen BR, Alexander EK, Bible KC, Doherty GM, Mandel SJ, Nikiforov YE, et al. 2015 American Thyroid Association Management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: the American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid. 2016;26:1–133. doi: 10.1089/thy.2015.0020. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources