

The Arteria Lymphatica and Lymphatic Microperforators: A Dedicated Blood Supply to Collecting Lymphatics and Their Potential Implications in Lymphedema: Anatomical Description
- PMID: 38268719
- PMCID: PMC10807887
- DOI: 10.1097/GOX.0000000000005547
The Arteria Lymphatica and Lymphatic Microperforators: A Dedicated Blood Supply to Collecting Lymphatics and Their Potential Implications in Lymphedema: Anatomical Description
Abstract
Background: Lymphedema is common after lymphatic damage in cancer treatment, with negative impacts on function and quality of life. Evidence suggests that blood vessel microvasculature is sensitive to irradiation and trauma; however, despite knowledge regarding dedicated mural blood supply to arteries and veins (vasa vasorum), equivalent blood vessels supplying lymphatics have not been characterized. We studied collecting lymphatics for dedicated mural blood vessels in our series of 500 lymphaticovenous anastomosis procedures for lymphedema, and equivalent controls.
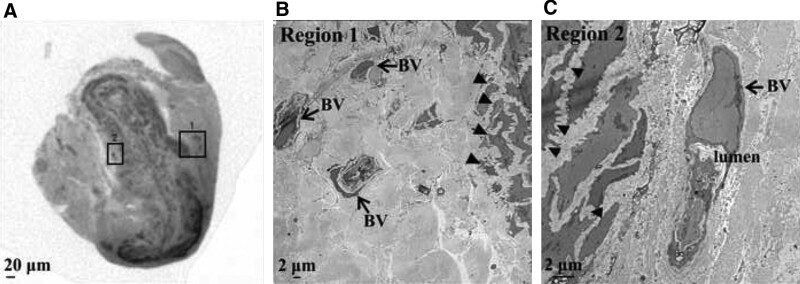
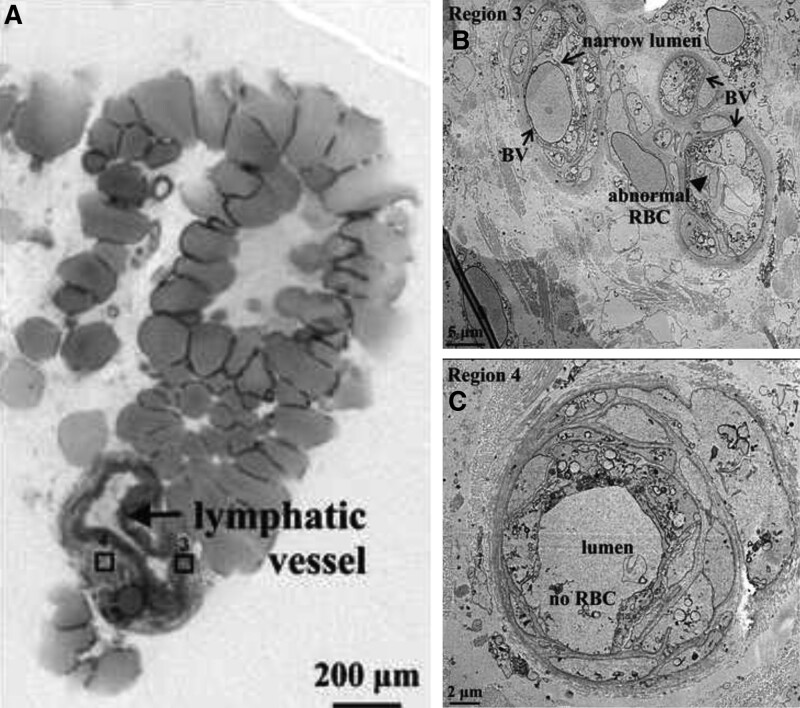
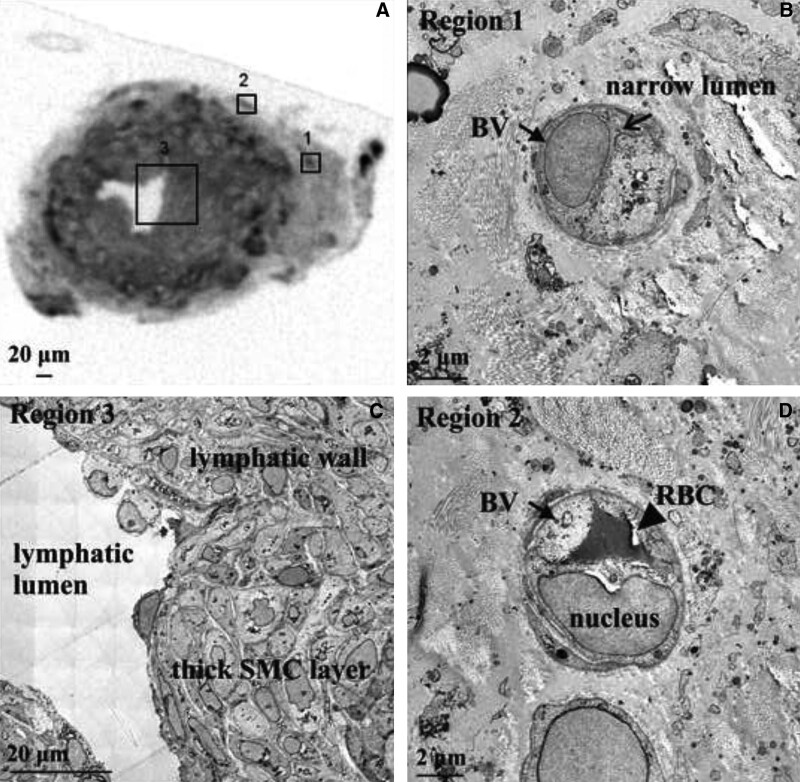
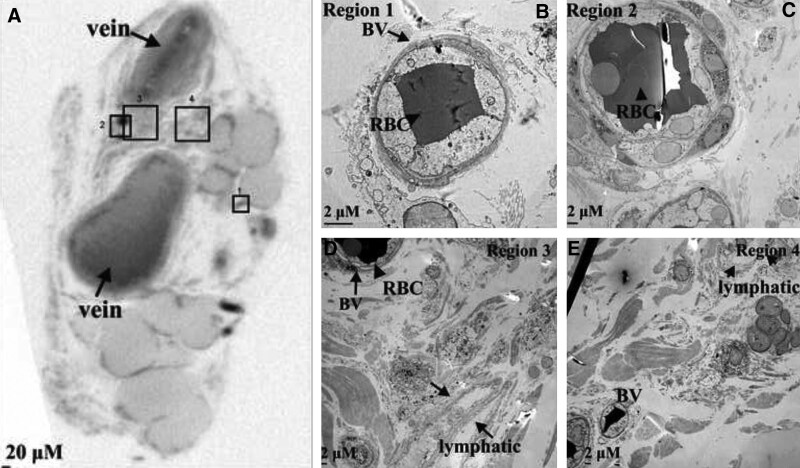
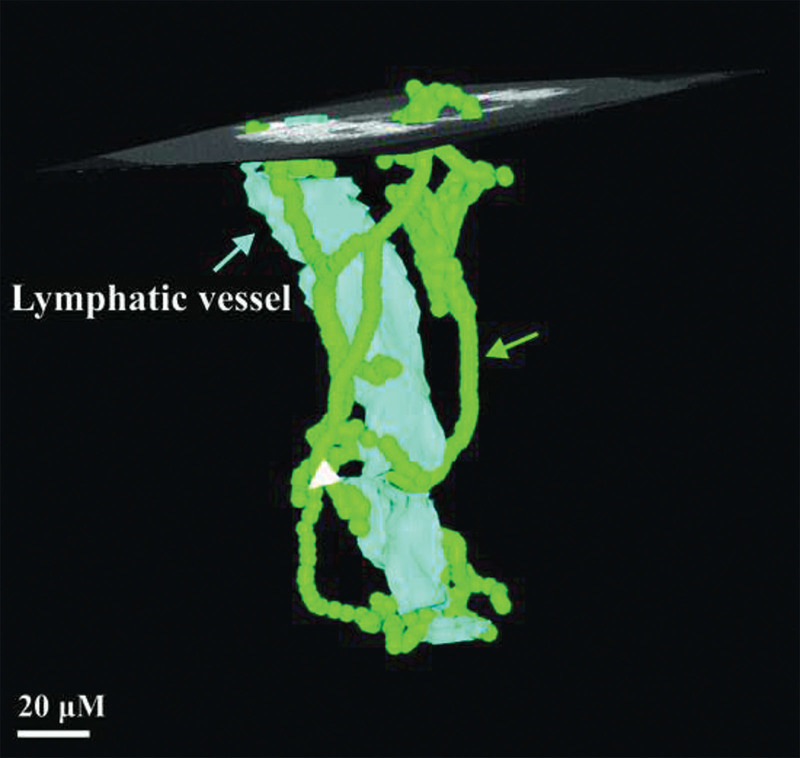
Methods: Microscopic images of lymphatics from lymphedema and control patients were analyzed for lymphatic wall vascular density. Collecting lymphatics from 20 patients with lymphedema and 10 control patients were sampled for more detailed analysis (podoplanin immunostaining, light/confocal microscopy, microcomputed tomography, and transmission electron microscopy) to assess lymphatic wall ultrastructure and blood supply.
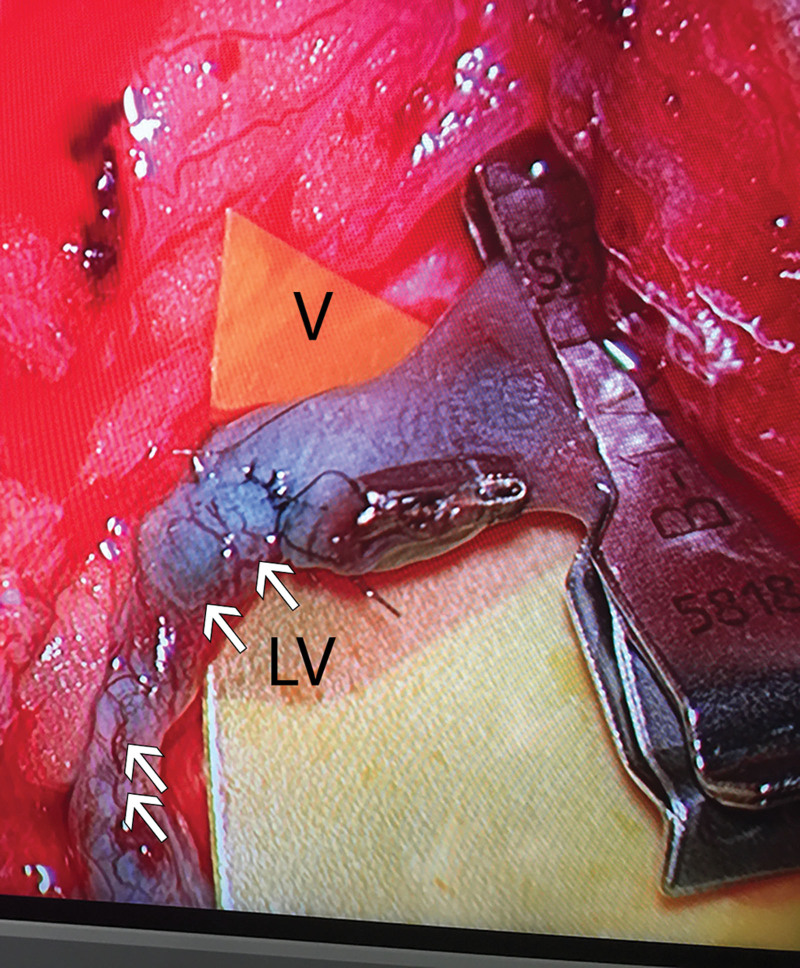
Results: Analysis revealed elaborate, dense blood microvessel networks associating with lymphatic walls in lymphedema patients and smaller equivalent vessels in controls. These vasa vasora or "arteria lymphatica" were supplied by regular axial blood vessels, parallel to lymphatic microperforators linking dermal and collecting lymphatics. Lymphatic walls were thicker in lymphedema patients than controls, with immunohistochemistry, computed tomography, transmission electron microscopy, and confocal microscopy characterizing abnormal blood vessels (altered appearance, thickened walls, elastin loss, narrow lumina, and fewer red blood cells) on these lymphatic walls.
Conclusions: Dedicated blood vessels on lymphatics are significantly altered in lymphedema. A better understanding of the role of these vessels may reveal mechanistic clues into lymphedema pathophysiology and technical aspects of lymphedema microsurgery, and suggest potential novel therapeutic targets.
Copyright © 2024 The Authors. Published by Wolters Kluwer Health, Inc. on behalf of The American Society of Plastic Surgeons.
Conflict of interest statement
Dr. Bendon received funding from the University of Melbourne and the Royal College of Surgeons of England. The other authors have no financial interest to declare. The work was funded by grants from The Stafford Fox and Wicking Trusts, Australia.
Figures

Similar articles
-
Vasa vasorum of superficial collecting lymphatics of human thigh.Lymphology. 1997 Sep;30(3):116-21. Lymphology. 1997. PMID: 9313203
-
Anatomy and function of the lymphatic vessels in the parietal pleura and their plasticity under inflammation in mice.Microvasc Res. 2023 Jul;148:104546. doi: 10.1016/j.mvr.2023.104546. Epub 2023 May 23. Microvasc Res. 2023. PMID: 37230165
-
New Insights into the Pathophysiology of Primary and Secondary Lymphedema: Histopathological Studies on Human Lymphatic Collecting Vessels.Lymphat Res Biol. 2020 Dec;18(6):502-509. doi: 10.1089/lrb.2020.0037. Epub 2020 Jul 20. Lymphat Res Biol. 2020. PMID: 32716244
-
Lymphatic Collecting Vessels in Health and Disease: A Review of Histopathological Modifications in Lymphedema.Lymphat Res Biol. 2022 Oct;20(5):468-477. doi: 10.1089/lrb.2021.0090. Epub 2022 Jan 17. Lymphat Res Biol. 2022. PMID: 35041535 Free PMC article. Review.
-
Mechanical forces and lymphatic transport.Microvasc Res. 2014 Nov;96:46-54. doi: 10.1016/j.mvr.2014.07.013. Epub 2014 Aug 5. Microvasc Res. 2014. PMID: 25107458 Free PMC article. Review.
References
-
- Mortimer PS. The pathophysiology of lymphedema. Cancer. 1998;83:2798–2802. - PubMed
-
- Oliver G, Detmar M. The rediscovery of the lymphatic system: old and new insights into the development and biological function of the lymphatic vasculature. Genes Dev. 2002;16:773–783. - PubMed
-
- Shayan R, Achen MG, Stacker SA. Lymphatic vessels in cancer metastasis: bridging the gaps. Carcinogenesis. 2006;27:1729–1738. - PubMed
-
- Johnson LA, Jackson DG. Control of dendritic cell trafficking in lymphatics by chemokines. Angiogenesis. 2014;17:335–345. - PubMed
LinkOut - more resources
Full Text Sources