

Characterizing a new clinical phenotype: the co-existence of cerebral venous outflow and connective tissue disorders
- PMID: 38269002
- PMCID: PMC10806170
- DOI: 10.3389/fneur.2023.1305972
Characterizing a new clinical phenotype: the co-existence of cerebral venous outflow and connective tissue disorders
Abstract
Background: There is increasing recognition of connective tissue disorders and their influence on disease in the general population. A conserved clinical phenotype involving connective tissue disorders and idiopathic intracranial hypertension (IIH) and associated cerebral venous outflow disorders (CVD) has not been previously described.
Methods: A single-institution retrospective review of a prospectively maintained database of patients with connective tissue disorders and CVD was performed.
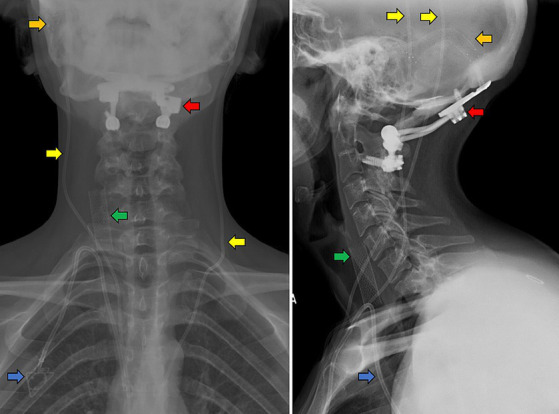
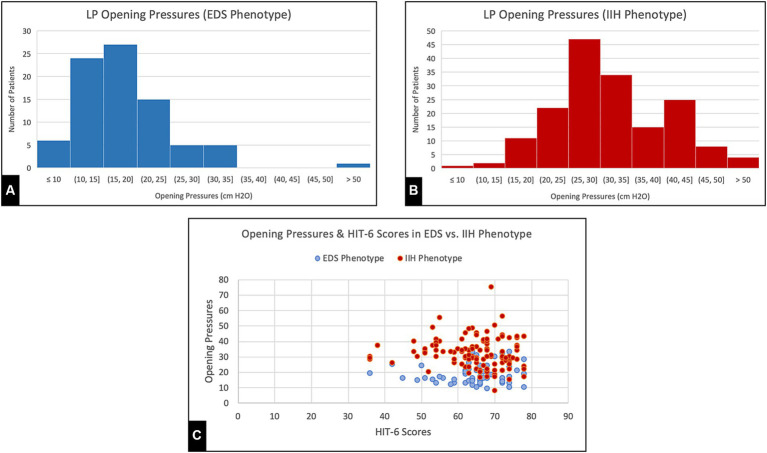
Results: A total of 86 patients were identified. The majority of these patients carried a diagnosis of Ehlers-Danlos syndrome (55%) and most were non-obese (mean body mass index 29.7 kg/m2), Caucasian (90%) females (87%). Most prevalent presenting symptoms included pressure headache (98%), dizziness (90%), tinnitus (92%), and cognitive dysfunction (69%). Aside from CVD and IIH, the most common associated conditions were postural orthostatic tachycardia syndrome (POTS; 55.8%), cerebrospinal fluid (CSF) leaks (51.2%), dysautonomia (45.3%), cranio-cervical instability (37.2%), mast cell activation syndrome (25.6%), and tethered cord syndrome (23.3%). Allergies to medications (87.2%) and surgical tape (19.8%) were also frequent. Despite significantly lower opening pressures on lumbar puncture, headache severity and quality of life scores were reported with the same severity of classic IIH patients, suggesting an underlying hypersensitivity to intracranial pressures and cerebral venous congestion.
Conclusion: There is a rare but conserved clinical phenotype that has not been described previously that presents with severe IIH symptoms in predominantly young, non-obese Caucasian women with a high associated incidence of dysautonomia, POTS, craniocervical instability, and CSF leaks, among others.
Keywords: Ehlers-Danlos; cerebral; connective; disorder; hypermobility; idiopathic; phenotype; tissue.
Copyright © 2024 Midtlien, Curry, Chang, Kiritsis, Aldridge and Fargen.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Scerrati A, Norri N, Mongardi L, Dones F, Ricciardi L, Trevisi G, et al. Styloidogenic-cervical spondylotic internal jugular venous compression, a vascular disease related to several clinical neurological manifestations: diagnosis and treatment—a comprehensive literature review. Ann Transl Med. (2021) 9:718. doi: 10.21037/atm-20-7698, PMID: - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources