

Cerebrospinal fluid ctDNA testing shows an advantage over plasma ctDNA testing in advanced non-small cell lung cancer patients with brain metastases
- PMID: 38269023
- PMCID: PMC10806520
- DOI: 10.3389/fonc.2023.1322635
Cerebrospinal fluid ctDNA testing shows an advantage over plasma ctDNA testing in advanced non-small cell lung cancer patients with brain metastases
Abstract
Background: Brain metastases (BM), including brain parenchyma metastases (BPM) and leptomeningeal metastases (LM), are devastating metastatic complications in advanced cancer patients. Next-generation sequencing (NGS) is emerging as a new promising tool for profiling cancer mutation, which could facilitate the diagnosis of cancer. This retrospective study aimed to investigate the molecular genetic characteristics of non-small cell lung cancer (NSCLC) patients with BPM and LM using NGS.
Methods: Cerebrospinal fluid (CSF) samples and paired plasma samples were collected from 37 patients of NSCLC-BM. We profiled genetic mutation characteristics using NGS from NSCLC-BM by comparing CSF circulating tumour DNA (ctDNA) with plasma ctDNA and primary tumour tissues.
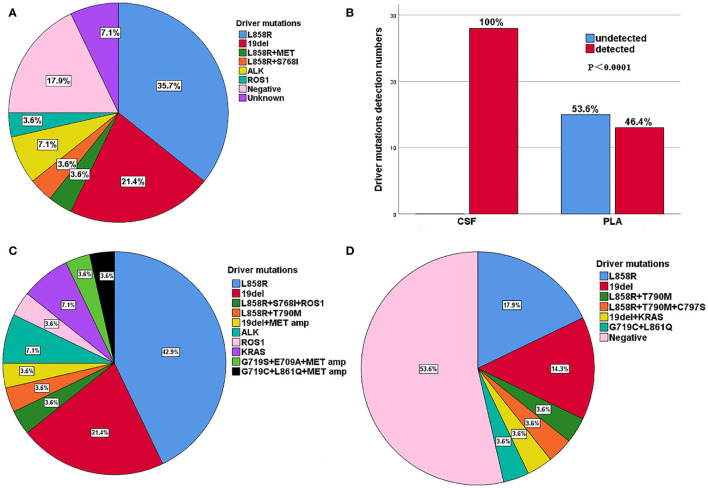
Results: Among the 37 patients with NSCLC-BM, 28 patients had LM with or without BPM, while 9 patients only had BPM. Driver and drug-resistant mutations in primary tumours with LM included: EGFR L858R (10, 35.7%), EGFR 19del (6, 21.4%), EGFR L858R+MET (1, 3.6%), EGFR L858R+S768I (1, 3.6%), ALK (2, 7.1%), ROS1 (1, 3.6%), negative (5, 17.9%), and unknown (2, 7.1%). In patients with NSCLC-LM, the detection rate and abundance of ctDNA in the CSF were significantly higher than those in paired plasma. The main driver mutations of NSCLC-LM remained highly consistent with those of the primary tumours, along with other unique mutations. Circulating tumour DNA was negative in the CSF samples of BPM patients. Patients with BMP had a higher ratio of EGFR 19del than L858R mutation (55.6% vs 11.1.%), whereas NSCLC patients with LM had a higher ratio of EGFR L858R than 19del mutation (50.0% vs 25.0%). Most patients with positive plasma ctDNA results were male (p = 0.058) and in an unstable state (p = 0.003).
Conclusion: Our study indicated that the CSF ctDNA detected by NGS may reflect the molecular characteristics and heterogeneity of NSCLC-LM. Timely screening of patients with NSCLC for CSF ctDNA, especially for patients with positive plasma ctDNA, may facilitate the early detection of LM. Furthermore, patients with the EGFR 19del may have a higher risk of developing BPM.
Keywords: brain parenchyma metastases (BPM); cerebrospinal fluid circulating tumour DNA (ctDNA); leptomeningeal metastases (LM); next generation sequencing; non-small cell lung cancer (NSCLC).
Copyright © 2024 Liu, Mei, Fang, Jia, Zhou, Li, Tian, Lu and Li.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures



References
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous