

Cystatin C or creatinine for pre-operative assessment of kidney function and risk of post-operative acute kidney injury: a secondary analysis of the METS cohort study
- PMID: 38269033
- PMCID: PMC10807905
- DOI: 10.1093/ckj/sfae004
Cystatin C or creatinine for pre-operative assessment of kidney function and risk of post-operative acute kidney injury: a secondary analysis of the METS cohort study
Abstract
Background: Post-operative acute kidney injury (PO-AKI) is a common surgical complication consistently associated with subsequent morbidity and mortality. Prior kidney dysfunction is a major risk factor for PO-AKI, however it is unclear whether serum creatinine, the conventional kidney function marker, is optimal in this population. Serum cystatin C is a kidney function marker less affected by body composition and might provide better prognostic information in surgical patients.
Methods: This was a pre-defined, secondary analysis of a multi-centre prospective cohort study of pre-operative functional capacity. Participants were aged ≥40 years, undergoing non-cardiac surgery. We assessed the association of pre-operative estimated glomerular filtration rate (eGFR) calculated using both serum creatinine and serum cystatin C with PO-AKI within 3 days after surgery, defined by KDIGO creatinine changes. The adjusted analysis accounted for established AKI risk factors.
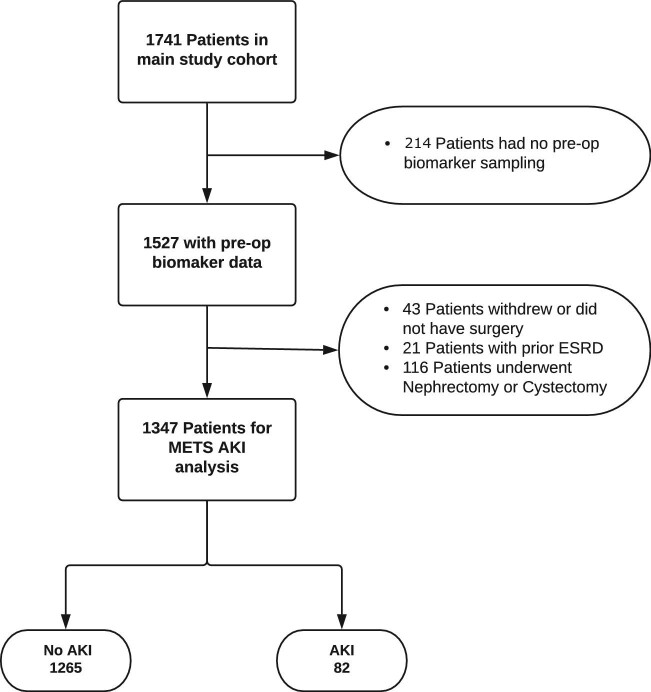
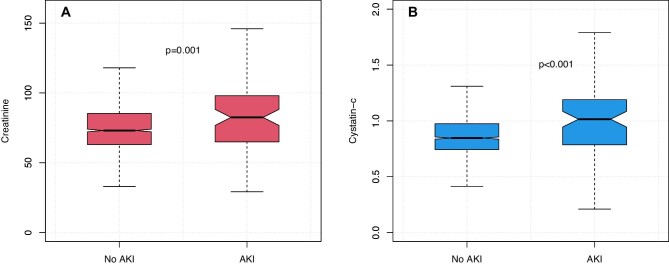
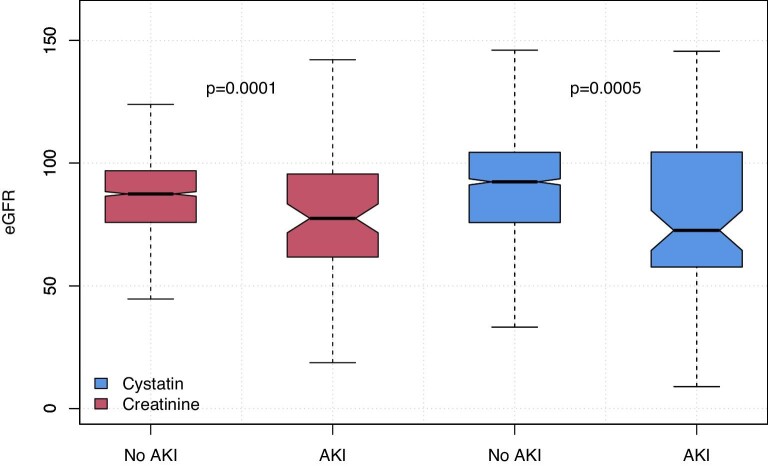
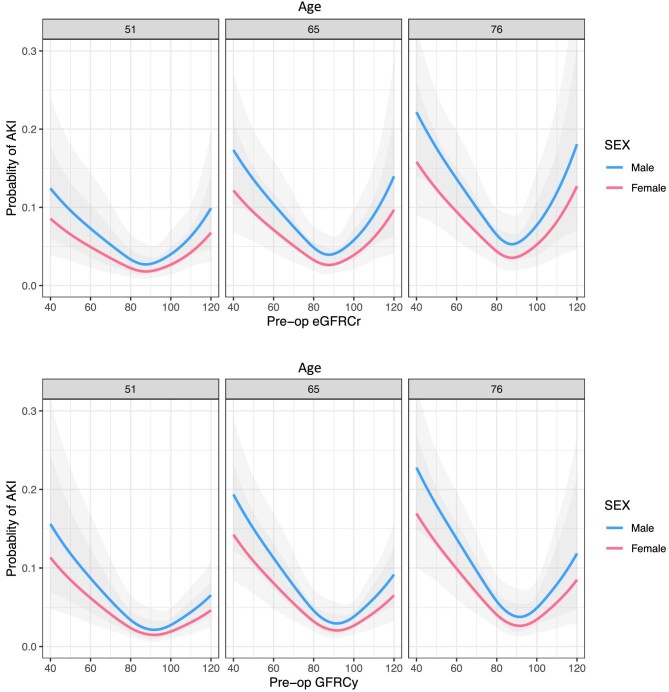
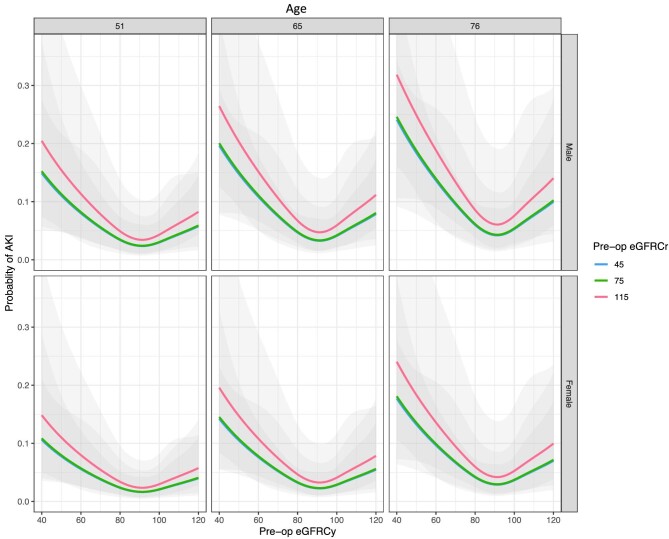
Results: A total of 1347 participants were included (median age 65 years, interquartile range 56-71), of whom 775 (58%) were male. A total of 82/1347 (6%) patients developed PO-AKI. These patients were older, had higher prevalence of cardiovascular disease and related medication, were more likely to have intra-abdominal procedures, had more intraoperative transfusion, and were more likely to be dead at 1 year after surgery 6/82 (7.3%) vs 33/1265 (2.7%) (P = .038). Pre-operative eGFR was lower in AKI than non-AKI patients using both creatinine and cystatin C. When both measurements were considered in a single age- and sex-adjusted model, eGFR-Cysc was strongly associated with PO-AKI, with increasing risk of AKI as eGFR-Cysc decreased below 90, while eGFR-Cr was no longer significantly associated.
Conclusions: Data from over 1000 prospectively recruited surgical patients confirms pre-operative kidney function as major risk factor for PO-AKI. Of the kidney function markers available, compared with creatinine, cystatin C had greater strength of association with PO-AKI and merits further assessment in pre-operative assessment of surgical risk.
Keywords: AKI; creatinine; cystatin C; prognosis; surgery.
© The Author(s) 2024. Published by Oxford University Press on behalf of the ERA.
Conflict of interest statement
J.R.P. has received honoraria from Paion Ltd, Baxter Inc., Biomerieux SA and Nikkiso Europe GmbH; he is a scientific advisor for Mission Therapeutics Ltd, Jafron Biomedical Co. Ltd and Nephrolyx GmbH, and serves on a Data Monitoring and Safety Board for Novartis Inc.; he is a specialty editor for the Clinical Kidney Journal and Blood Purification. B.H.C. and D.N.W. are supported in part by Merit Awards from the Department of Anesthesiology and Pain Medicine at the University of Toronto. D.N.W. is supported in part by the Endowed Chair in Translational Anesthesiology Research at St Michael's Hospital and the University of Toronto. D.N.W. has received honoraria from Edwards Lifesciences within the last 5 years and is a member of the Scientific Advisory Board for Surgical Safety Technologies Inc. T.E.F.A. is an NIHR Clinical Lecturer, an editor of the British Journal of Anaesthesia, has received research funding from the Medical Research Council, the National Institute of Academic Anaesthesia and Barts Charity, and has received consultancy fees from MSD and Edwards Life Sciences unrelated to this work. All other authors report no financial relationships with any organizations that might have an interest in the submitted work in the previous 3 years, and no other relationships or activities that could appear to have influenced the submitted work.
Figures
References
-
- Weiser TG, Haynes AB, Molina Get al. Estimate of the global volume of surgery in 2012: an assessment supporting improved health outcomes. Lancet 2015;385:S11. http://www.ncbi.nlm.nih.gov/pubmed/26313057 - PubMed
-
- Fowler AJ, Abbott TEF, Prowle Jet al. Age of patients undergoing surgery. Br J Surg 2019;106:1012–8. https://www.ncbi.nlm.nih.gov/pubmed/31115918 - PubMed
-
- Abbott TEF, Fowler AJ, Dobbs TDet al. Frequency of surgical treatment and related hospital procedures in the UK: a national ecological study using hospital episode statistics. Br J Anaesth 2017;119:249–57. https://www.ncbi.nlm.nih.gov/pubmed/28854546 - PubMed
-
- Lei VJ, Luong T, Shan Eet al. Risk stratification for postoperative acute kidney injury in major noncardiac surgery using preoperative and intraoperative data. JAMA Netw Open 2019;2:e1916921. https://www.ncbi.nlm.nih.gov/pubmed/31808922 - PMC - PubMed
-
- Grams ME, Sang Y, Coresh Jet al. Acute kidney injury after major surgery: a retrospective analysis of Veterans Health Administration data. Am J Kidney Dis 2016;67:872–80. http://www.ncbi.nlm.nih.gov/pubmed/26337133 - PMC - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
