

A Multinational Case Series Describing Successful Treatment of Persistent Severe Acute Respiratory Syndrome Coronavirus 2 Infection Caused by Omicron Sublineages With Prolonged Courses of Nirmatrelvir/Ritonavir
- PMID: 38269048
- PMCID: PMC10807981
- DOI: 10.1093/ofid/ofad612
A Multinational Case Series Describing Successful Treatment of Persistent Severe Acute Respiratory Syndrome Coronavirus 2 Infection Caused by Omicron Sublineages With Prolonged Courses of Nirmatrelvir/Ritonavir
Abstract
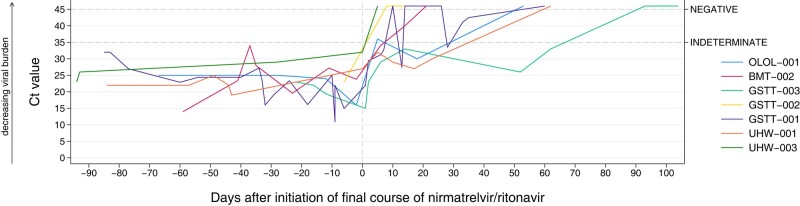
The optimum treatment for persistent infection with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) is not known. Our case series, across 5 hospitals in 3 countries, describes 11 cases where persistent SARS-CoV-2 infection was successfully treated with prolonged courses (median, 10 days [range, 10-18 days]) of nirmatrelvir/ritonavir (Paxlovid). Most cases (9/11) had hematological malignancy and 10 (10/11) had received CD20-depleting therapy. The median duration of infection was 103 days (interquartile range, 85-138 days). The majority (10/11) were hospitalized, and 7 (7/11) had severe/critical disease. All survived and 9 of 11 demonstrated viral clearance, almost half (4/9) of whom received nirmatrelvir/ritonavir as monotherapy. This case series suggests that prolonged nirmatrelvir/ritonavir has a role in treating persistent infection.
Keywords: COVID-19; Immunocompromise; SARS-CoV-2.
© The Author(s) 2023. Published by Oxford University Press on behalf of Infectious Diseases Society of America.
Conflict of interest statement
Potential conflicts of interest. All authors: No reported conflicts.
Figures
References
-
- Agarwal A, Rochwerg B, Lamontagne F, et al. . A living WHO guideline on drugs for covid-19. BMJ 2020; 370:m3379. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
