

Extended Induction and Prognostic Indicators of Response in Patients Treated with Mirikizumab with Moderately to Severely Active Ulcerative Colitis in the LUCENT Trials
- PMID: 38271613
- PMCID: PMC11630349
- DOI: 10.1093/ibd/izae004
Extended Induction and Prognostic Indicators of Response in Patients Treated with Mirikizumab with Moderately to Severely Active Ulcerative Colitis in the LUCENT Trials
Abstract
Background: Efficacy and safety of mirikizumab, a p19-targeted anti-interleukin-23 monoclonal antibody, for moderately to severely active ulcerative colitis was demonstrated previously. We evaluated clinical response, baseline characteristics, and clinical status in patients not responding by 12 weeks (W) of induction who then received extended induction treatment.
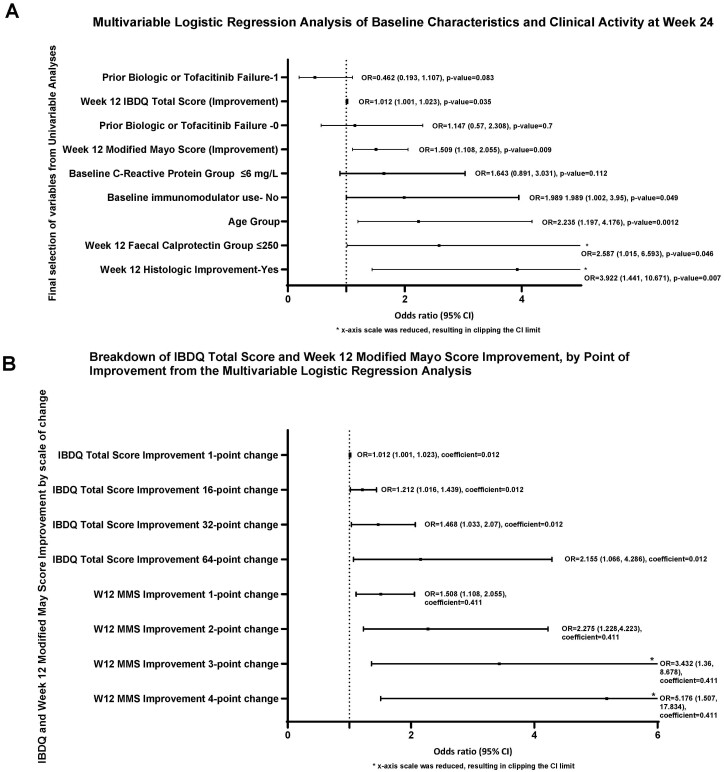
Method: Patients unresponsive to 300 mg of intravenous (IV) mirikizumab every 4 weeks by W12 received 3 additional 300 mg IV doses every 4 weeks. Week-4 responders received 200 mg mirikizumab every 4 weeks subcutaneously until W52. Patients responding by W12 but subsequently losing response received rescue therapy with 300 mg IV for 3 doses every 4 weeks. Logistic regression modelling was performed for patients not achieving W12 clinical response to assess baseline characteristics and W12 efficacy parameters and potential prognostic factors of clinical response at W24.
Results: Of patients not achieving clinical response during induction, 53.7% achieved response following extended induction. After 52W, 72.2%, 43.1%, and 36.1% of patients achieved clinical response, endoscopic, and clinical remission, respectively. Of induction responders who subsequently lost response, 63.2% and 36.8% achieved symptomatic response and remission, respectively, after receiving rescue therapy No prior biologic or tofacitinib treatment, no immunomodulators at baseline, age older than 40 years, and W12 modified Mayo Score improvement were positively associated with a response to extended induction. The safety profile was similar to initial induction, with 38.3% treatment emergent adverse events, mostly mild.
Conclusion: With "extended induction," total of 80.3% mirikizumab-treated patients achieved clinical response by W24. Potential prognostic factors determining response include disease severity, disease phenotype, C-reactive protein, and previous biologic therapy.
Keywords: IL-23 antibodies; extended induction; mirikizumab; ulcerative colitis.
Plain language summary
Extended induction with mirikizumab led to clinical response in more than half of primary nonresponders. Intravenous reinduction therapy in patients losing response during treatment led to more than 60% achieving symptomatic response, confirming the clinical benefit of these treatment strategies for harder to treat patients.
© 2024 Crohn’s & Colitis Foundation. Published by Oxford University Press on behalf of Crohn’s & Colitis Foundation.
Conflict of interest statement
G.D’H. reports advisor fees from AbbVie, Alimentiv, AstraZeneca, Boehringer Ingelheim, Bristol-Myers Squibb, Celltrion, Eli Lilly and Company, Galapagos, GlaxoSmithKline, Gossamerbio, Pfizer, Immunic, Johnson and Johnson, Takeda, Prometheus Biosciences, Prometheus Laboratories, Protagonist, Samsung, Seres, Tillotts, and Ventyx.
P.H. reports consulting fees from AbbVie, Buhlmann Labs, Celltrion, Eli Lilly and Company, Takeda.
L.P-B. reports consulting fees from AbbVie, Alimentiv, Alma Bio Therapeutics, Amgen, Applied Molecular Transport, Arena, Biogen, BMS, Celltrion, CONNECT Biopharm, Cytoki Pharma, Enthera, Ferring, Fresenius Kabi, Galapagos, Genentech, Gilead, Gossamer Bio, GSK, HAC-Pharma, IAG Image Analysis, Index Pharmaceuticals, Inotrem, Janssen, Lilly, Medac, Mopac, Morphic, MSD, Norgine, Novartis, OM Pharma, ONO Pharma, OSE Immunotherapeutics, Pandion Therapeutics, Par’Immune, Pfizer, Prometheus, Protagonist, Roche, Sanofi, Sandoz, Takeda, Theravance, Thermo Fisher, Tigenix, Tillots, Viatris, Vifor, Ysopia, Abivax, Samsung, Ventyx, Roivant, Vectivbio; grants from Takeda, Fresenius Kabi, Celltrion; lecture fees from Galapagos, AbbVie, Janssen, Genentech, Ferring, Tillots, Celltrion, Takeda, Pfizer, Sandoz, Biogen, MSD, Amgen, Vifor, Arena, Lilly, Gilead, Viatris, and Medac.
B.E.S. reports consulting fees from Abbvie, Alimentiv, Amgen, Arena Pharmaceuticals, Artugen Therapeutics, Astra Zeneca, Boehringer Ingelheim, Boston Pharmaceuticals, Calibr, Celgene, Celltrion, ClostraBio, Equillium, Enthera, Evommune, Fresenius Kabi, Galapagos, Genentech (Roche), Gilead Sciences, GlaxoSmithKline, Gossamer Bio, Index Pharmaceuticals, Innovation Pharmaceuticals, Inotrem, Kaleido, Kallyope, Merck, Morphic Therapeutics, MRM Health, Progenity, Prometheus Biosciences, Prometheus Laboratories, Protagonist Therapeutics, Q32 Bio, Sun Pharma, Surrozen, Target RWE, Teva, TLL Pharmaceutical, and Ventyx Biosciences; consulting and speaking fees from Abivax; consulting and speaking fees and other support from Lilly; research grants, consulting and speaking fees and other support from Bristol Myers Squibb, Janssen, Pfizer, Takeda; research grants and consulting fees from Theravance Biopharma; and stock options from Ventyx Biopharma.
S.B. reports receives grant and research support from the following: AbbVie Pharmaceuticals, UCB Pharma, Janssen Pharmaceuticals, Inc, Salix Pharmaceuticals, Takeda Pharmaceuticals, Inc, Celgene Pharmaceuticals, Inc, Pfizer Pharmaceuticals, Inc, Atlantic Pharmaceuticals, Ltd., Gilead Sciences, Inc, Tetherex Pharmaceuticals, Arena Pharmaceuticals, and Shield Therapeutics PLC and has consulted for UCB Pharma, Mesoblast, Cornerstones, Janssen Pharmaceuticals, Inc, Takeda Pharmaceuticals, Inc, Arena Pharmaceuticals, Eli Lilly and Company, Celgene Pharmaceuticals, Inc, Celltrion Healthcare Co, Ltd, Pfizer Pharmaceuticals, and Salix Pharmaceuticals.
T.K. has served as a speaker, a consultant, or an advisory board member for AbbVie, Alfresa Pharma, Bristol Myers Squibb, Celltrion, Covidien, EA Pharma, Eiken chemical, Eli Lilly, Ferring Pharmaceuticals, Gilead Sciences, Janssen, JIMRO, Kissei, Kyorin Pharmaceutical, Mitsubishi Tanabe Pharma, Mochida Pharmaceutical, Nippon Kayaku, Pfizer, Sekisui Medical, Takeda Pharmaceutical, and Zeria Pharmaceutical and received research funding from AbbVie, Alfresa Pharma, EA Pharma, Kyorin Pharmaceutical, Mochida Pharmaceutical, Nippon Kayaku, Otsuka Holdings, Pfizer, Sekisui Medical, and Zeria Pharmaceutical.
A.K. reports being an Eli Lilly and Company contract employee.
R.E.M., I.R., R.E., T.H.G., N.M., X.Z., and V.A. all report being an Eli Lilly and Company employee and stockholder.
Figures




References
-
- Sands BE, Chen J, Penney M, et al.830 Initial evaluation of MEDI2070 (specific anti-IL-23 antibody) in patients with active Crohn’s disease who have failed anti-TNF antibody therapy: a randomized, double-blind placebo-controlled phase 2A induction study. Gastroenterology. 2015;148(4):S-163.
-
- Ben-Horin S, Chowers Y.. Tailoring anti-TNF therapy in IBD: drug levels and disease activity. Nat Rev Gastroenterol Hepatol. 2014;11(4):243-255. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
