

Endoscopic and clinical features of gastric emphysema
- PMID: 38273039
- PMCID: PMC10810885
- DOI: 10.1038/s41598-024-52633-z
Endoscopic and clinical features of gastric emphysema
Abstract
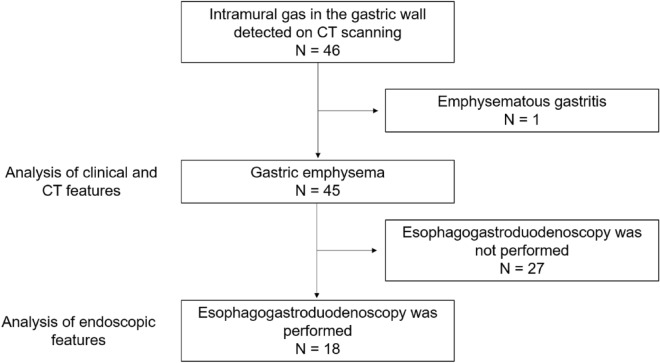
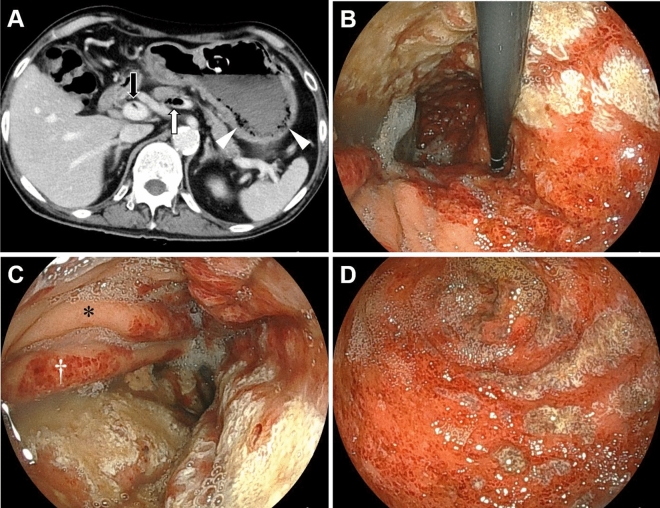
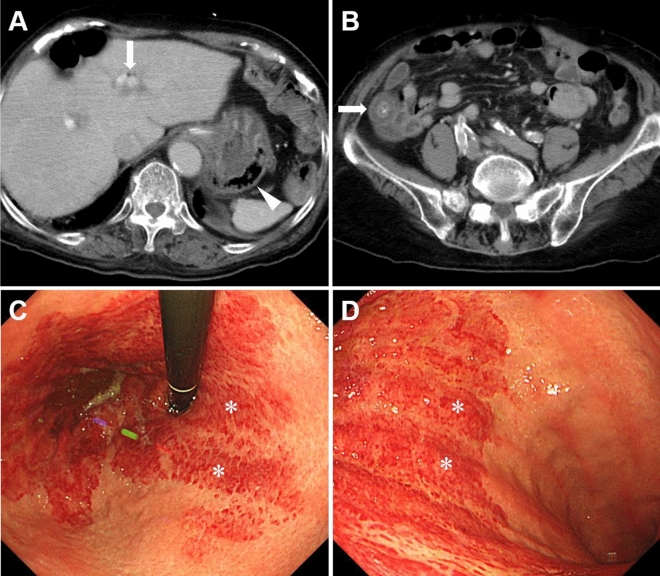
Gastric emphysema is characterized by the presence of intramural gas in the stomach without bacterial infection. Due to its rarity, most reports on gastric emphysema have been limited to single-case studies, and this condition's clinical and endoscopic features have not been thoroughly investigated. In this study, we analyzed 45 patients with gastric emphysema from 10 institutions and examined their characteristics, endoscopic features, and outcomes. The mean age at diagnosis of gastric emphysema in our study population (35 males and 10 females) was 68.6 years (range, 14-95 years). The top five underlying conditions associated with gastric emphysema were the placement of a nasogastric tube (26.7%), diabetes mellitus (20.0%), post-percutaneous endoscopic gastrostomy (17.8%), malignant neoplasms (17.8%), and renal failure (15.6%). Among the 45 patients, 42 were managed conservatively with fasting and administration of proton pump inhibitors. Unfortunately, seven patients died within 30 days of diagnosis, and 35 patients experienced favorable recoveries. The resolution of gastric emphysema was confirmed in 30 patients through computed tomography (CT) scans, with a mean duration of 17.1 ± 34.9 days (mean ± standard deviation [SD], range: 1-180 days) from the time of diagnosis to the disappearance of the gastric intramural gas. There were no instances of recurrence. Endoscopic evaluation was possible in 18 patients and revealed that gastric emphysema presented with features such as redness, erosion, coarse mucosa, and ulcers, with fewer mucosal injuries on the anterior wall (72.2%), a clear demarcation between areas of mucosal injury and intact mucosa (61.1%), and predominantly longitudinal mucosal injuries on the stomach folds (50.0%). This study is the first English-language report to analyze endoscopic findings in patients with gastric emphysema.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
