

Development of an image-based Random Forest classifier for prediction of surgery duration of laparoscopic sigmoid resections
- PMID: 38273097
- PMCID: PMC10811180
- DOI: 10.1007/s00384-024-04593-z
Development of an image-based Random Forest classifier for prediction of surgery duration of laparoscopic sigmoid resections
Abstract
Purpose: Sigmoid diverticulitis is a disease with a high socioeconomic burden, accounting for a high number of left-sided colonic resections worldwide. Modern surgical scheduling relies on accurate prediction of operation times to enhance patient care and optimize healthcare resources. This study aims to develop a predictive model for surgery duration in laparoscopic sigmoid resections, based on preoperative CT biometric and demographic patient data.
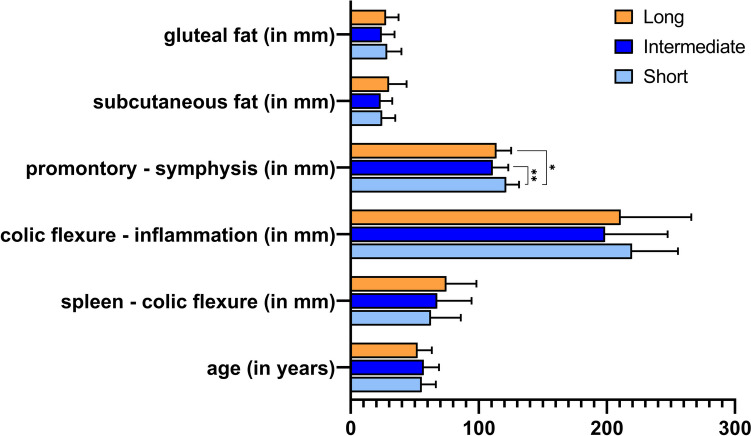
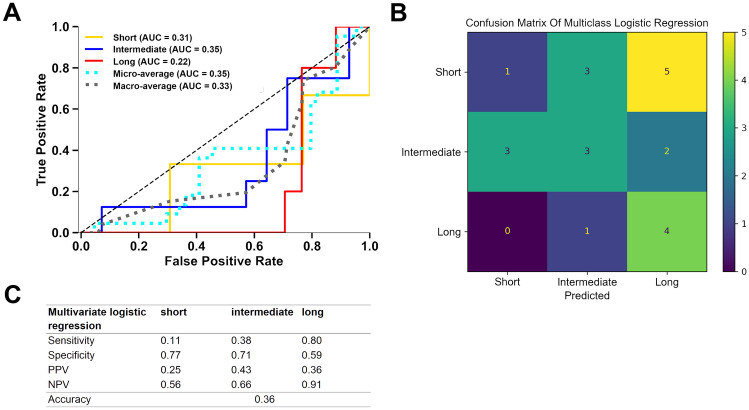
Methods: This retrospective single-center cohort study included 85 patients who underwent laparoscopic sigmoid resection for diverticular disease. Potentially relevant procedure-specific anatomical parameters recommended by a surgical expert were measured in preoperative CT imaging. After random split into training and test set (75% / 25%) multiclass logistic regression was performed and a Random Forest classifier was trained on CT imaging parameters, patient age, and sex in the training cohort to predict categorized surgery duration. The models were evaluated in the test cohort using established performance metrics including receiver operating characteristics area under the curve (AUROC).
Results: The Random Forest model achieved a good average AUROC of 0.78. It allowed a very good prediction of long (AUROC = 0.89; specificity 0.71; sensitivity 1.0) and short (AUROC = 0.81; specificity 0.77; sensitivity 0.56) procedures. It clearly outperformed the multiclass logistic regression model (AUROC: average = 0.33; short = 0.31; long = 0.22).
Conclusion: A Random Forest classifier trained on demographic and CT imaging biometric patient data could predict procedure duration outliers of laparoscopic sigmoid resections. Pending validation in a multicenter study, this approach could potentially improve procedure scheduling in visceral surgery and be scaled to other procedures.
Keywords: Computed tomography; Diverticulitis; Laparoscopic surgery; Machine learning; Random Forest; Surgery scheduling.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- Peery AF, Dellon ES, Lund J, Crockett SD, McGowan CE, Bulsiewicz WJ, Gangarosa LM, Thiny MT, Stizenberg K, Morgan DR, Ringel Y, Kim HP, DiBonaventura MD, Carroll CF, Allen JK, Cook SF, Sandler RS, Kappelman MD, Shaheen NJ (2012) Burden of gastrointestinal disease in the United States: 2012 update. Gastroenterology 143(5):1179–1187.e3 - PMC - PubMed
-
- Sartelli M, Weber DG, Kluger Y, Ansaloni L, Coccolini F, Abu-Zidan F, Augustin G, Ben-Ishay O, Biffl WL, Bouliaris K, Catena R, Ceresoli M, Chiara O, Chiarugi M, Coimbra R, Cortese F, Cui Y, Damaskos D, Angelis GL, de’ Delibegovic S, Demetrashvili Z, de Simone B, Di Marzo F, Di Saverio S, Duane TM, Faro MP, Fraga GP, Gkiokas G, Gomes CA, Hardcastle TC, Hecker A, Karamarkovic A, Kashuk J, Khokha V, Kirkpatrick AW, Kok KYY, Inaba K, Isik A, Labricciosa FM, Latifi R, Leppäniemi A, Litvin A, Mazuski JE, Maier RV, Marwah S, McFarlane M, Moore EE, Moore FA, Negoi I, Pagani L, Rasa K, Rubio-Perez I, Sakakushev B, Sato N, Sganga G, Siquini W, Tarasconi A, Tolonen M, Ulrych J, Zachariah SK, Catena F (2020) 2020 update of the WSES guidelines for the management of acute colonic diverticulitis in the emergency setting. World J Emerg Surg 15(1):32 - PMC - PubMed
-
- Guller U, Jain N, Hervey S, Purves H, Pietrobon R (2003) Laparoscopic vs open colectomy: outcomes comparison based on large nationwide databases. Arch Surg (Chicago, Ill.: 1960) 138(11):1179–1186 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
