

Evaluating the Impact of Enhanced Recovery After Surgery Protocols on Surgical Outcomes Following Bariatric Surgery-A Systematic Review and Meta-analysis of Randomised Clinical Trials
- PMID: 38273146
- PMCID: PMC10899423
- DOI: 10.1007/s11695-024-07072-0
Evaluating the Impact of Enhanced Recovery After Surgery Protocols on Surgical Outcomes Following Bariatric Surgery-A Systematic Review and Meta-analysis of Randomised Clinical Trials
Abstract
Background: Enhanced recovery after surgery (ERAS) programmes are evidence-based care improvement processes for surgical patients, which are designed to decrease the impact the anticipated negative physiological cascades following surgery.
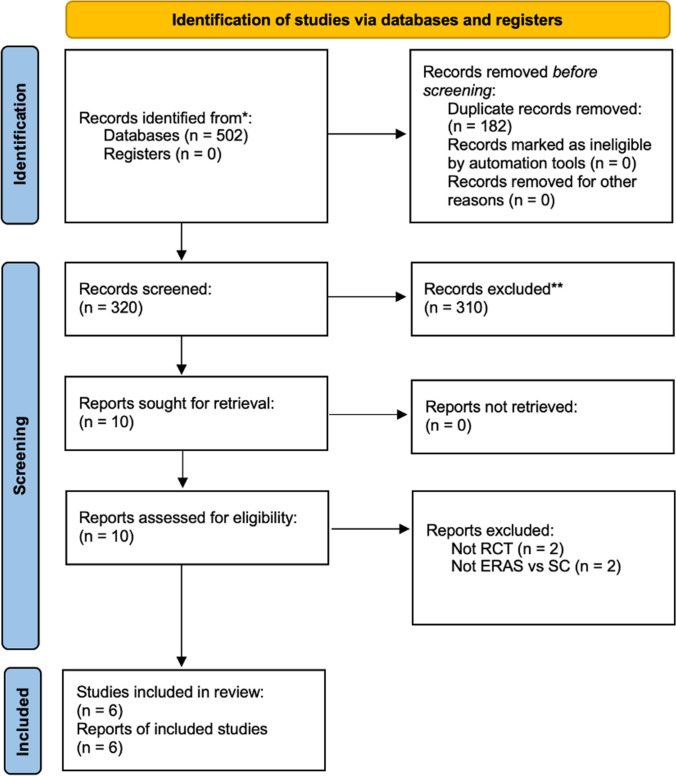
Aim: To perform a systematic review and meta-analysis of randomised clinical trials (RCTs) to evaluate the impact of ERAS protocols on outcomes following bariatric surgery compared to standard care (SC).
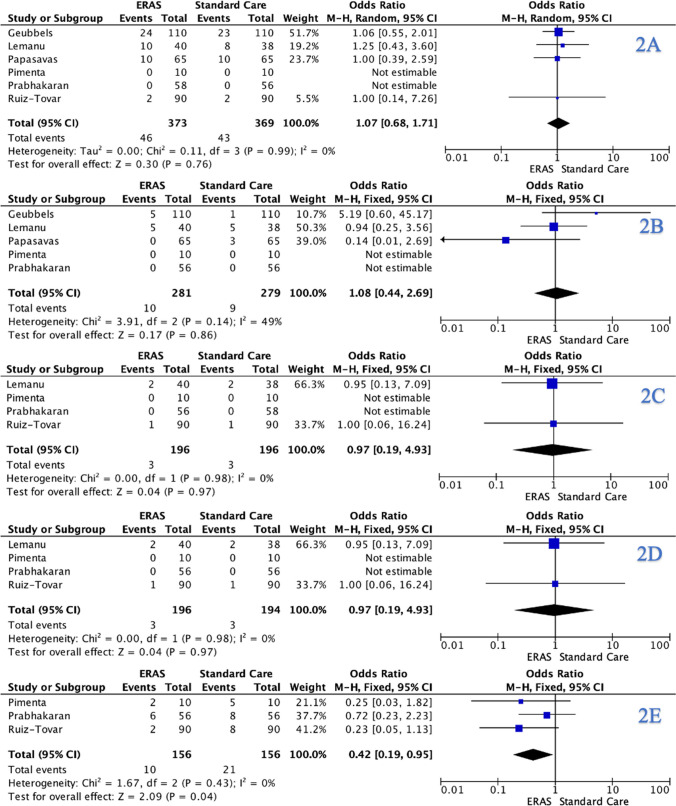
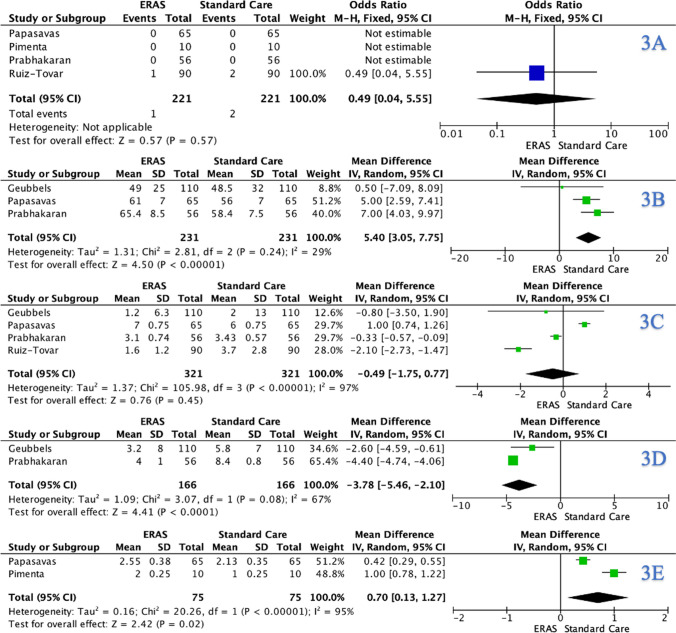
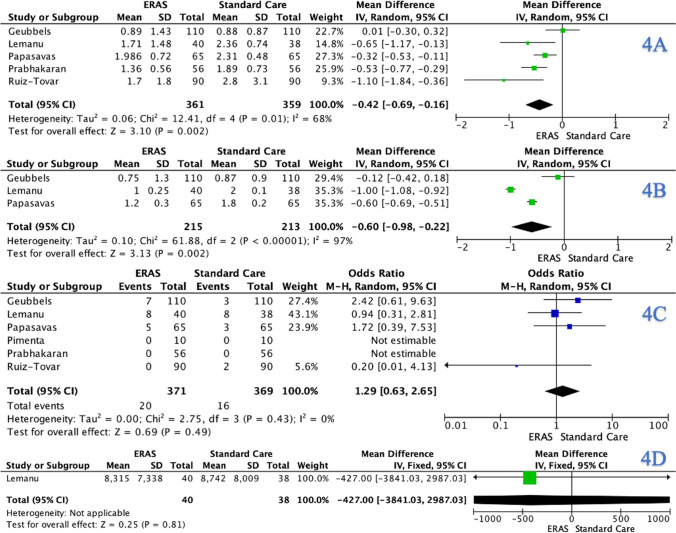
Methods: A systematic review was performed in accordance with PRISMA guidelines. Meta-analysis was performed using Review Manager version 5.4 RESULTS: Six RCTs including 740 patients were included. The mean age was 40.2 years, and mean body mass index was 44.1 kg/m2. Overall, 54.1% underwent Roux-en-Y gastric bypass surgery (400/740) and 45.9% sleeve gastrectomy (340/700). Overall, patients randomised to ERAS programmes had a significant reduction in nausea and vomiting (odds ratio (OR): 0.42, 95% confidence interval (CI): 0.19-0.95, P = 0.040), intraoperative time (mean difference (MD): 5.40, 95% CI: 3.05-7.77, P < 0.001), time to mobilisation (MD: - 7.78, 95% CI: - 5.46 to - 2.10, P < 0.001), intensive care unit stay (ICUS) (MD: 0.70, 95% CI: 0.13-1.27, P = 0.020), total hospital stay (THS) (MD: - 0.42, 95% CI: - 0.69 to - 0.16, P = 0.002), and functional hospital stay (FHS) (MD: - 0.60, 95% CI: - 0.98 to - 0.22, P = 0.002) compared to those who received SC.
Conclusion: ERAS programmes reduce postoperative nausea and vomiting, intraoperative time, time to mobilisation, ICUS, THS, and FHS compared to those who received SC. Accordingly, ERAS should be implemented, where feasible, for patients indicated to undergo bariatric surgery. Trial registration International Prospective Register of Systematic Reviews (PROSPERO - CRD42023434492.
Keywords: Bariatric surgery; ERAS; Enhanced recovery after surgery; Patient outcomes.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Evaluating the impact of enhanced recovery after surgery protocols following oesophagectomy: a systematic review and meta-analysis of randomised clinical trials.Dis Esophagus. 2025 Jan 7;38(1):doae118. doi: 10.1093/dote/doae118. Dis Esophagus. 2025. PMID: 39791389 Free PMC article.
-
Enhanced Recovery after Surgery (ERAS): a Systematic Review of Randomised Controlled Trials (RCTs) in Bariatric Surgery.Obes Surg. 2020 Dec;30(12):5071-5085. doi: 10.1007/s11695-020-05000-6. Epub 2020 Sep 26. Obes Surg. 2020. PMID: 32981000
-
Evaluating the impact of enhanced recovery after surgery protocols following emergency laparotomy - A systematic review and meta-analysis of randomised clinical trials.Am J Surg. 2024 Oct;236:115857. doi: 10.1016/j.amjsurg.2024.115857. Epub 2024 Jul 18. Am J Surg. 2024. PMID: 39098254
-
Impact of implementation of an enhanced recovery after surgery (ERAS) program in laparoscopic Roux-en-Y gastric bypass: a prospective randomized clinical trial.Surg Obes Relat Dis. 2019 Feb;15(2):228-235. doi: 10.1016/j.soard.2018.11.002. Epub 2018 Nov 14. Surg Obes Relat Dis. 2019. PMID: 30606469 Clinical Trial.
-
Outcomes of Enhanced Recovery After Surgery Protocols Versus Conventional Management in Patients Undergoing Bariatric Surgery.J Laparoendosc Adv Surg Tech A. 2022 Feb;32(2):176-182. doi: 10.1089/lap.2020.0783. Epub 2021 May 14. J Laparoendosc Adv Surg Tech A. 2022. PMID: 33989060
Cited by
-
Evaluating the impact of enhanced recovery after surgery protocols following oesophagectomy: a systematic review and meta-analysis of randomised clinical trials.Dis Esophagus. 2025 Jan 7;38(1):doae118. doi: 10.1093/dote/doae118. Dis Esophagus. 2025. PMID: 39791389 Free PMC article.
-
Enhanced Recovery After Bariatric Surgery and Admission to the Intensive Care Unit: A Potential Paradox.Obes Surg. 2025 Aug;35(8):2785-2786. doi: 10.1007/s11695-025-07990-7. Epub 2025 Jun 24. Obes Surg. 2025. PMID: 40553317 No abstract available.
-
Experiencing Complications After Metabolic and Bariatric Surgeries is a Risk Factor for Postoperative Emergency Department Admissions: a Retrospective Cohort Study.Obes Surg. 2025 Mar;35(3):875-883. doi: 10.1007/s11695-025-07710-1. Epub 2025 Feb 1. Obes Surg. 2025. PMID: 39891838 Free PMC article.
-
Risk factors as criteria for drain use in gastrectomy: A prospective study.Mol Clin Oncol. 2025 Jun 26;23(2):75. doi: 10.3892/mco.2025.2870. eCollection 2025 Aug. Mol Clin Oncol. 2025. PMID: 40630940 Free PMC article.
-
Effect of the enhanced recovery after surgery protocol in patients undergoing elective craniotomies: a systematic review and meta-analysis.Neurosurg Rev. 2025 Mar 10;48(1):291. doi: 10.1007/s10143-025-03446-9. Neurosurg Rev. 2025. PMID: 40063290
References
-
- Finucane MM, Stevens GA, Cowan MJ, et al. National, regional, and global trends in body-mass index since 1980: systematic analysis of health examination surveys and epidemiological studies with 960 country-years and 9·1 million participants. Lancet. 2011;377(9765):557–567. doi: 10.1016/S0140-6736(10)62037-5. - DOI - PMC - PubMed
-
- Ng M, Fleming T, Robinson M, et al. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2014;384(9945):766–781. doi: 10.1016/S0140-6736(14)60460-8. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
