

Drug-Drug Interactions Between Glucagon-Like Peptide 1 Receptor Agonists and Oral Medications: A Systematic Review
- PMID: 38273155
- PMCID: PMC11018670
- DOI: 10.1007/s40264-023-01392-3
Drug-Drug Interactions Between Glucagon-Like Peptide 1 Receptor Agonists and Oral Medications: A Systematic Review
Abstract
Background: Glucagon-like peptide 1 receptor agonists (GLP1RAs) are used in the treatment of diabetes and obesity. Their slowing effect of gastric emptying might change oral drug absorption, potentially affecting pharmacokinetics, particularly in the case of medications with a narrow therapeutic index.
Purpose: The purpose of this systematic review is to summarize data on drug-drug interactions between GLP1RAs and oral drugs.
Data sources: The PubMed and EMBASE databases were searched up to November, 1st 2023.
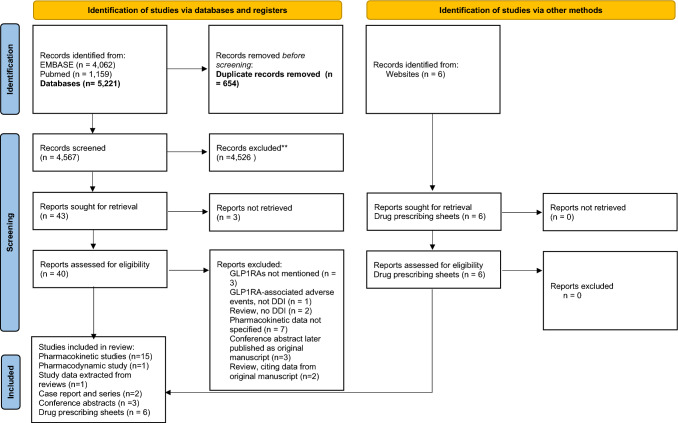
Study selection: We selected pharmacokinetic studies of any injectable GLP1RA given with an oral medication, and product prescribing sheets reporting data without access to the original study.
Data extraction: Two authors independently extracted the data.
Data synthesis: Twenty-two reports and six prescribing sheets were included. Treatment with GLP1RAs resulted in unaffected or reduced Cmax and delayed tmax of drugs with high solubility and permeability (warfarin, contraceptive pills, acetaminophen), drugs with high solubility and low permeability (angiotensin converting enzyme inhibitors), drugs with low solubility and high permeability (statins) and drugs with low solubility and permeability (digoxin). However, the use of GLP1RAs did not exert clinically significant changes in the AUC or differences in clinically relevant endpoints.
Limitations: The major limitations of the studies that are included in this systematic review are the enrollment of healthy subjects and insufficient data in conditions that might affect pharmacokinetics (e.g., kidney dysfunction).
Conclusions: To conclude, reduced Cmax and delayed tmax of drugs co-administered with GLP1RAs are consistent with the known delayed gastric output by the latter. Nevertheless, the overall drug exposure was not considered clinically significant. Dose adjustments are probably not required for simultaneous use of GLP1RAs with oral medications. Still, results should be carefully generalized to cases of background kidney dysfunction or when using drugs with narrow therapeutic index. The study is registered in PROSPERO: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42022332339 .
© 2024. The Author(s).
Conflict of interest statement
BC declares that there are no relationships or activities that might bias, or be perceived to bias, her work. ID has received fees from Astra Zeneca, Novo Nordisk, Abbott, Boehringer Ingleheim, Elli Lilly and Sanofi for educational lectures, and participated in advisory boards of Novo Nordisk, Boehringer Ingleheim, Sanofi and Novartis that are outside the scope of this work. ID reports a grant from Astra Zeneca that is outside the scope of the submitted work. DS declares that there are no relationships or activities that might bias, or be perceived to bias, his work. AL declares that there are no relationships or activities that might bias, or be perceived to bias, his work. TDC has received fees from Astra Zeneca for educational lectures that are outside the scope of this work.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
