

High Tyrosol and Hydroxytyrosol Intake Reduces Arterial Inflammation and Atherosclerotic Lesion Microcalcification in Healthy Older Populations
- PMID: 38275655
- PMCID: PMC10812987
- DOI: 10.3390/antiox13010130
High Tyrosol and Hydroxytyrosol Intake Reduces Arterial Inflammation and Atherosclerotic Lesion Microcalcification in Healthy Older Populations
Abstract
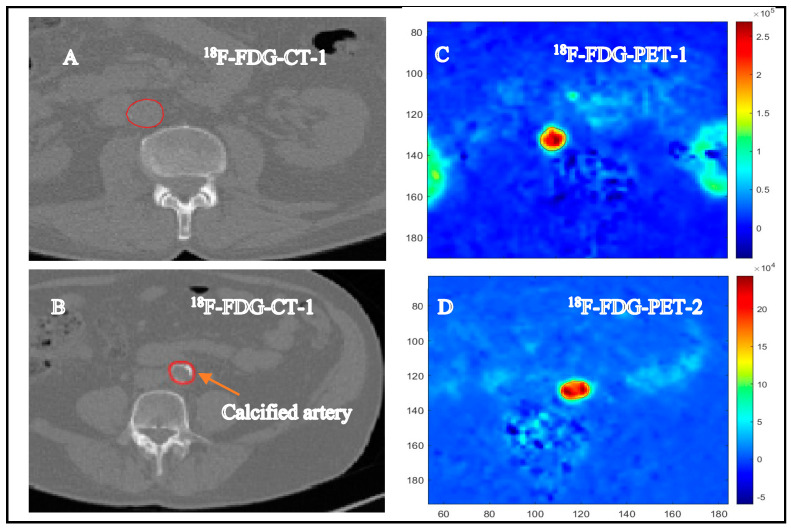
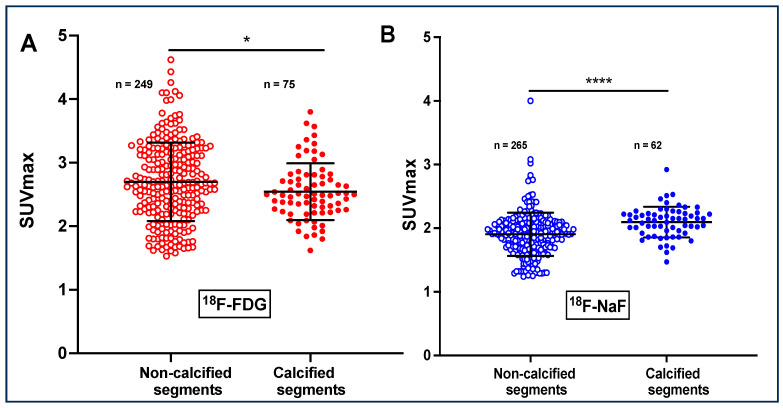
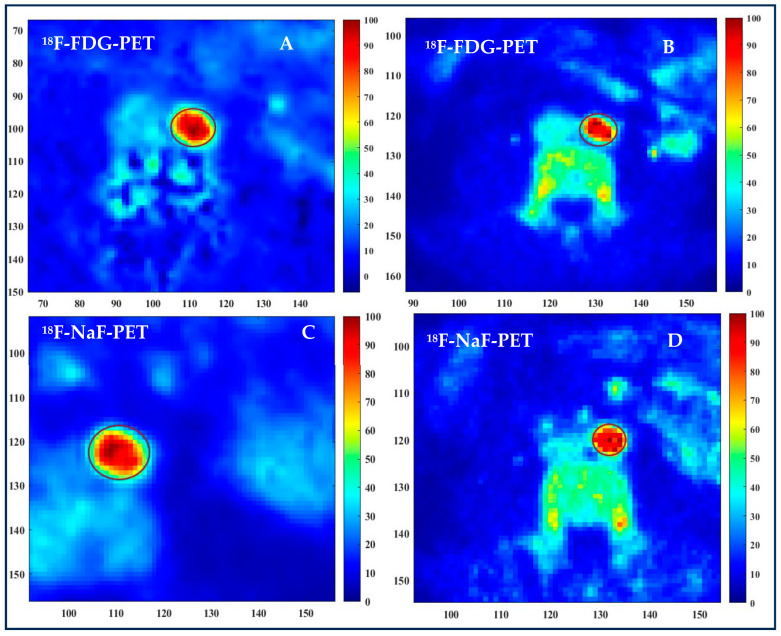
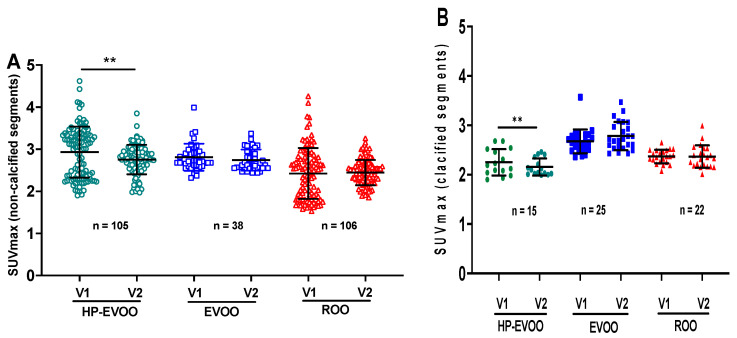
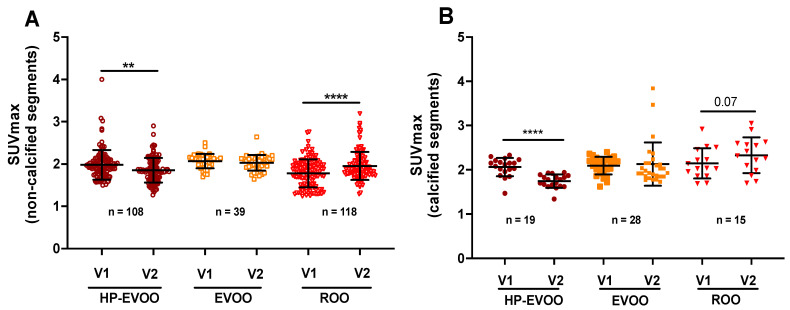
Aging is an important risk factor for cardiovascular diseases and convincing data have shown that chronic low-grade inflammation, which develops with advanced age, contributes significantly to cardiovascular risk. The present study aimed to use 18F-FDG/18F-NaF-PET/CT imaging to, respectively, gauge arterial inflammation and microcalcification in a healthy elderly population and to assess the potential benefits of a tyrosol- and hydroxytyrosol-rich diet on these two markers of atherosclerotic plaque fragility. Eleven healthy participants (mean age 75 ± 5.67 years) were supplemented for 6 months with high polyphenol-rich extra virgin olive oil (HP-EVOO), extra virgin olive oil (EVOO), or refined olive oil (ROO). The participants underwent PET/CT imaging with 18F-FDG and 18F-NaF radiotracers at baseline and after 6 months. 18F-FDG and 18F-NaF uptakes were quantified using standardized uptake values (SUV) and were categorized based on artery calcification and olive oil type. A total of 324 slices of the aortas of the imaged participants were analyzed for arterial inflammation and 327 slices were analyzed for microcalcification. 18F-FDG uptake was significantly higher in the non-calcified segments than in the calcified segments (SUVmax = 2.70 ± 0.62 and SUVmax = 2.54 ± 0.44, respectively, p < 0.042). Conversely, the non-calcified segments displayed significantly lower 18F-NaF uptake than the calcified segments (SUVmax = 1.90 ± 0.37 and 2.09 ± 0.24, respectively, p < 0.0001). The 6-month supplementation with HP-EVOO induced a significant reduction in 18F-FDG uptake in both the non-calcified (2.93 ± 0.23 to 2.75 ± 0.38, p < 0.004) and calcified segments of the aortas (2.25 ± 0.29 to 2.15 ± 0.19, p < 0.02). 18F-NaF uptake was also significantly lower in patients supplemented with HP-EVOO (SUVmax = 1.98 ± 0.33 at baseline compared to 1.85 ± 0.28, after the 6-month supplementation, p < 0.004), whereas no significant effect was observed with EVOO. Conversely, participants supplemented with ROO displayed a significant increase in 18F-NaF uptake (SUVmax = 1.78 ± 0.34 to 1.95 ± 0.34, p < 0.0001). The present study confirmed that a phenolic-compound-rich diet reduces both arterial inflammation and atherosclerotic lesion microcalcification and demonstrated that 18F-FDG/18F-NaF-PET/CT imaging is a valuable approach for assessing age-related arterial damage.
Keywords: 18F-FDG/18F-NaF; aging; atherosclerosis; hydroxytyrosol; positron emission tomography; tyrosol; vascular inflammation.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
Associations of subclinical microcalcification and inflammation with carotid atheroma development: a dual-tracer PET/CT study.Eur J Nucl Med Mol Imaging. 2025 Jun;52(7):2502-2512. doi: 10.1007/s00259-025-07127-z. Epub 2025 Feb 13. Eur J Nucl Med Mol Imaging. 2025. PMID: 39939531 Free PMC article.
-
Non-calcified active atherosclerosis plaque detection with 18F-NaF and 18F-FDG PET/CT dynamic imaging.Phys Eng Sci Med. 2023 Mar;46(1):295-302. doi: 10.1007/s13246-023-01218-7. Epub 2023 Jan 30. Phys Eng Sci Med. 2023. PMID: 36715851
-
Association Between Osteogenesis and Inflammation During the Progression of Calcified Plaque Evaluated by 18F-Fluoride and 18F-FDG.J Nucl Med. 2017 Jun;58(6):968-974. doi: 10.2967/jnumed.116.182790. Epub 2017 Feb 23. J Nucl Med. 2017. PMID: 28232606
-
Imaging Atherosclerosis by PET, With Emphasis on the Role of FDG and NaF as Potential Biomarkers for This Disorder.Front Physiol. 2020 Oct 22;11:511391. doi: 10.3389/fphys.2020.511391. eCollection 2020. Front Physiol. 2020. PMID: 33192540 Free PMC article. Review.
-
Targeted PET/CT imaging of vulnerable atherosclerotic plaques: microcalcification with sodium fluoride and inflammation with fluorodeoxyglucose.Curr Cardiol Rep. 2013 Jun;15(6):364. doi: 10.1007/s11886-013-0364-4. Curr Cardiol Rep. 2013. PMID: 23605466 Review.
Cited by
-
Improving the Biostability of Extra Virgin Olive Oil with Olive Fruit Extract During Prolonged Deep Frying.Foods. 2025 Jan 15;14(2):260. doi: 10.3390/foods14020260. Foods. 2025. PMID: 39856925 Free PMC article.
-
Extra Virgin Olive Oil and Metabolic Diseases.Int J Mol Sci. 2024 Jul 25;25(15):8117. doi: 10.3390/ijms25158117. Int J Mol Sci. 2024. PMID: 39125686 Free PMC article. Review.
-
Potential Therapeutic Properties of Olea europaea Leaves from Selected Cultivars Based on Their Mineral and Organic Profiles.Pharmaceuticals (Basel). 2024 Feb 22;17(3):274. doi: 10.3390/ph17030274. Pharmaceuticals (Basel). 2024. PMID: 38543060 Free PMC article.
-
Examination of Primary and Secondary Metabolites Associated with a Plant-Based Diet and Their Impact on Human Health.Foods. 2024 Mar 27;13(7):1020. doi: 10.3390/foods13071020. Foods. 2024. PMID: 38611326 Free PMC article. Review.
-
Dietary associations with reduced epigenetic age: a secondary data analysis of the methylation diet and lifestyle study.Aging (Albany NY). 2025 Apr 17;17(4):994-1010. doi: 10.18632/aging.206240. Epub 2025 Apr 17. Aging (Albany NY). 2025. PMID: 40266024 Free PMC article. Clinical Trial.
References
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
