

The Clinical, Genomic, and Transcriptomic Landscape of BRAF Mutant Cancers
- PMID: 38275886
- PMCID: PMC10814895
- DOI: 10.3390/cancers16020445
The Clinical, Genomic, and Transcriptomic Landscape of BRAF Mutant Cancers
Abstract
Background: BRAF mutations are classified into four molecularly distinct groups, and Class 1 (V600) mutant tumors are treated with targeted therapies. Effective treatment has not been established for Class 2/3 or BRAF Fusions. We investigated whether BRAF mutation class differed according to clinical, genomic, and transcriptomic variables in cancer patients.
Methods: Using the AACR GENIE (v.12) cancer database, the distribution of BRAF mutation class in adult cancer patients was analyzed according to sex, age, primary race, and tumor type. Genomic alteration data and transcriptomic analysis was performed using The Cancer Genome Atlas.
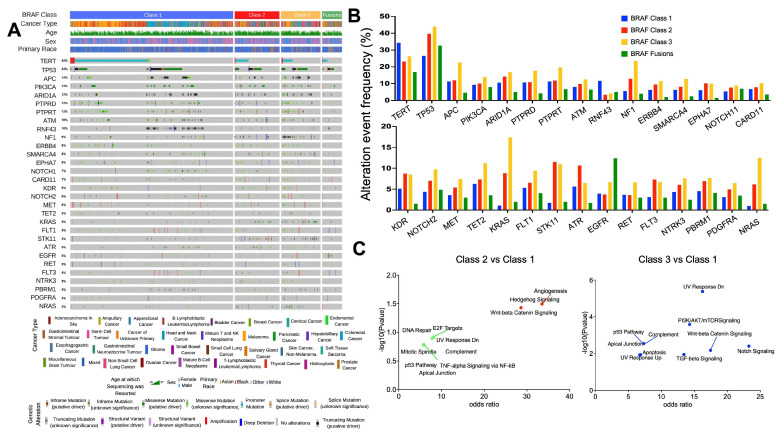
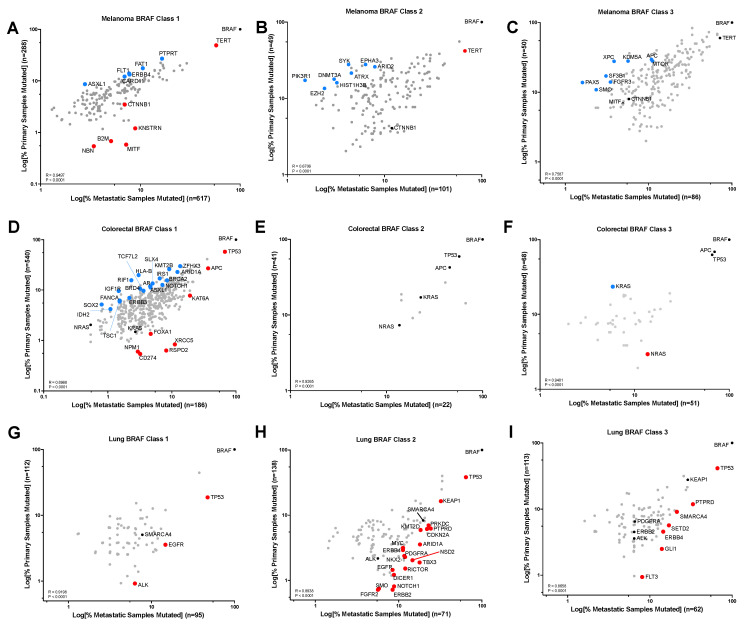
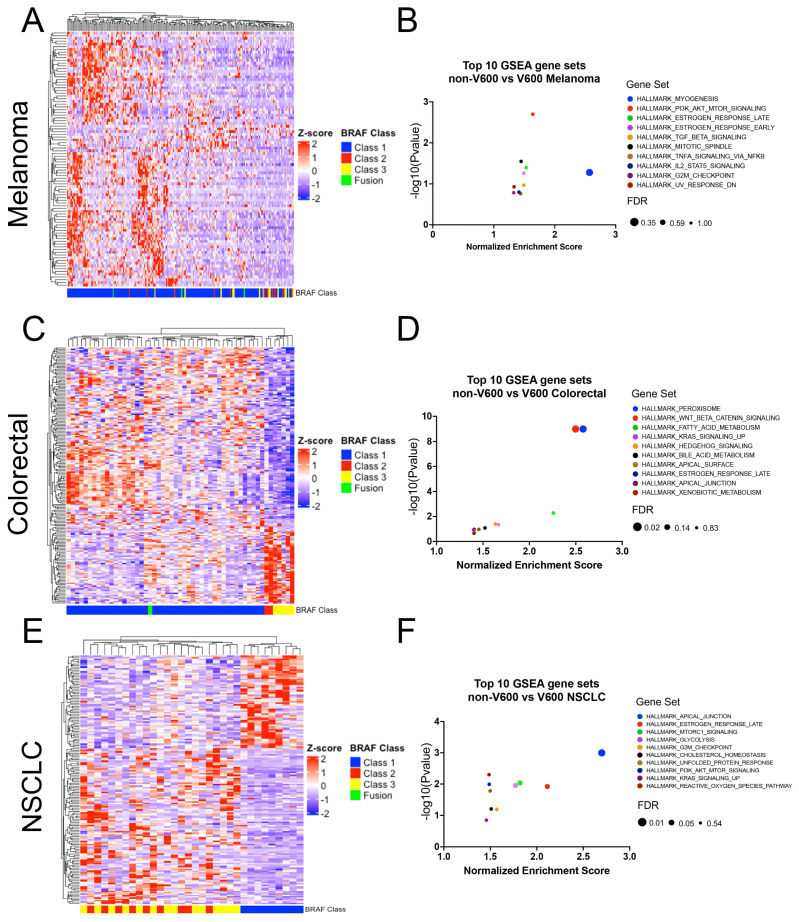
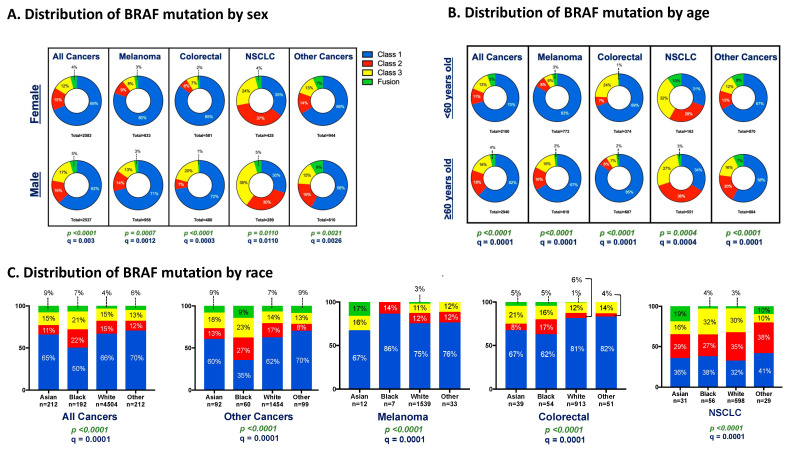
Results: BRAF mutations were identified in 9515 (6.2%) samples among 153,834, with melanoma (31%), CRC (20.7%), and NSCLC (13.9%) being the most frequent cancer types. Class 1 harbored co-mutations outside of the MAPK pathway (TERT, RFN43) vs. Class 2/3 mutations (RAS, NF1). Across all tumor types, Class 2/3 were enriched for alterations in genes involved in UV response and WNT/β-catenin. Pathway analysis revealed enrichment of WNT/β-catenin and Hedgehog signaling in non-V600 mutated CRC. Males had a higher proportion of Class 3 mutations vs. females (17.4% vs. 12.3% q = 0.003). Non-V600 mutations were generally more common in older patients (aged 60+) vs. younger (38% vs. 15% p < 0.0001), except in CRC (15% vs. 30% q = 0.0001). Black race was associated with non-V600 BRAF alterations (OR: 1.58; p < 0.0001).
Conclusions: Class 2/3 BRAFs are more present in Black male patients with co-mutations outside of the MAPK pathway, likely requiring additional oncogenic input for tumorigenesis. Improving access to NGS and trial enrollment will help the development of targeted therapies for non-V600 BRAF mutations.
Keywords: BRAF mutation; MAPK pathway; colorectal cancer; melanoma; non-small cell lung cancer.
Conflict of interest statement
The following authors declare the listed conflicts of interest: David W. Cescon —Consultancy advisory relationships with AstraZeneca, Daiichi Sankyo, Eisai, Gilead, GlaxoSmithKline, Inflex, Inivata/NeoGenomics, Lilly, Merck, Novartis, Pfizer, Roche and Saga; research funding to their institution from AstraZeneca, Guardant Health, Gilead, GlaxoSmithKline, Inivata/NeoGenomics, Knight, Merck, Pfizer, ProteinQure and Roche; and holds a patent (US62/675,228) for methods of treating cancers characterized by a high expression level of spindle and kinetochore associated complex subunit 3 (ska3) gene. Anna Spreafico—Honoraria: Bristol Myers Squibb, Medison & Immunocore. Consulting or Advisory Role: Novartis, Merck, Bristol Myers Squibb, Oncorus, Medison & Immunocore. Research Funding: Bristol Myers Squibb, Novartis, Merck, Symphogen, AstraZeneca/MedImmune, Bayer, Surface Oncology, Janssen Oncology, Northern Biologics, Replimune, Roche, Alkermes, Array BioPharma, GlaxoSmithKline, Treadwell Therapeutics (Inst), Amgen (Inst). Travel, Accommodations, Expenses: Merck, Bristol Myers Squibb, Idera, Bayer, Janssen Oncology, Roche. Gerald Batist — Partner in a Genome Canada proteomics grant with AstraZeneca. April A.N. Rose—Employment: Merck. Recipient: an immediate family member Stock and Other Ownership interests: Merck by an immediate family member. Consulting or Advisory Role: EMD Serono, Advanced Accelerator Applications/Novartis Research Funding: Canadian Institutes of Health Research (CIHR), Canadian Cancer Society, Conquer Cancer Foundation, Jewish General Hospital Foundation, TransMedTech Institute, Canada Foundation for Innovation, AstraZeneca Canada, Merck, Pfizer, Seattle Genetics. The remaining authors have no conflicts of interest to declare.
Figures
References
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
