

Role of Transjugular Intrahepatic Portosystemic Shunt in the Liver Transplant Setting
- PMID: 38276106
- PMCID: PMC10816519
- DOI: 10.3390/jcm13020600
Role of Transjugular Intrahepatic Portosystemic Shunt in the Liver Transplant Setting
Abstract
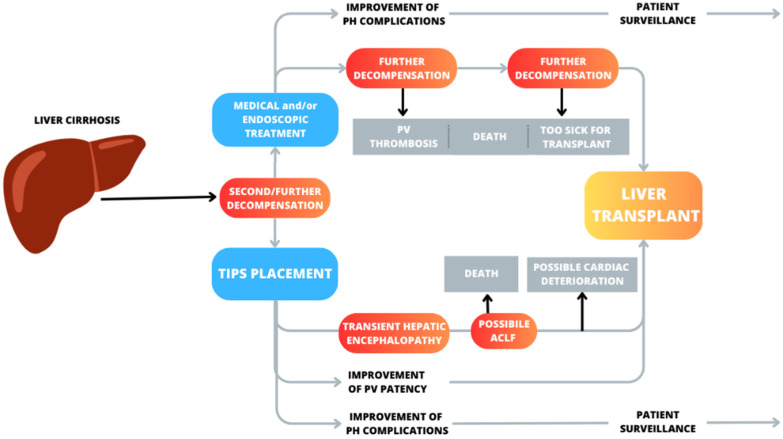
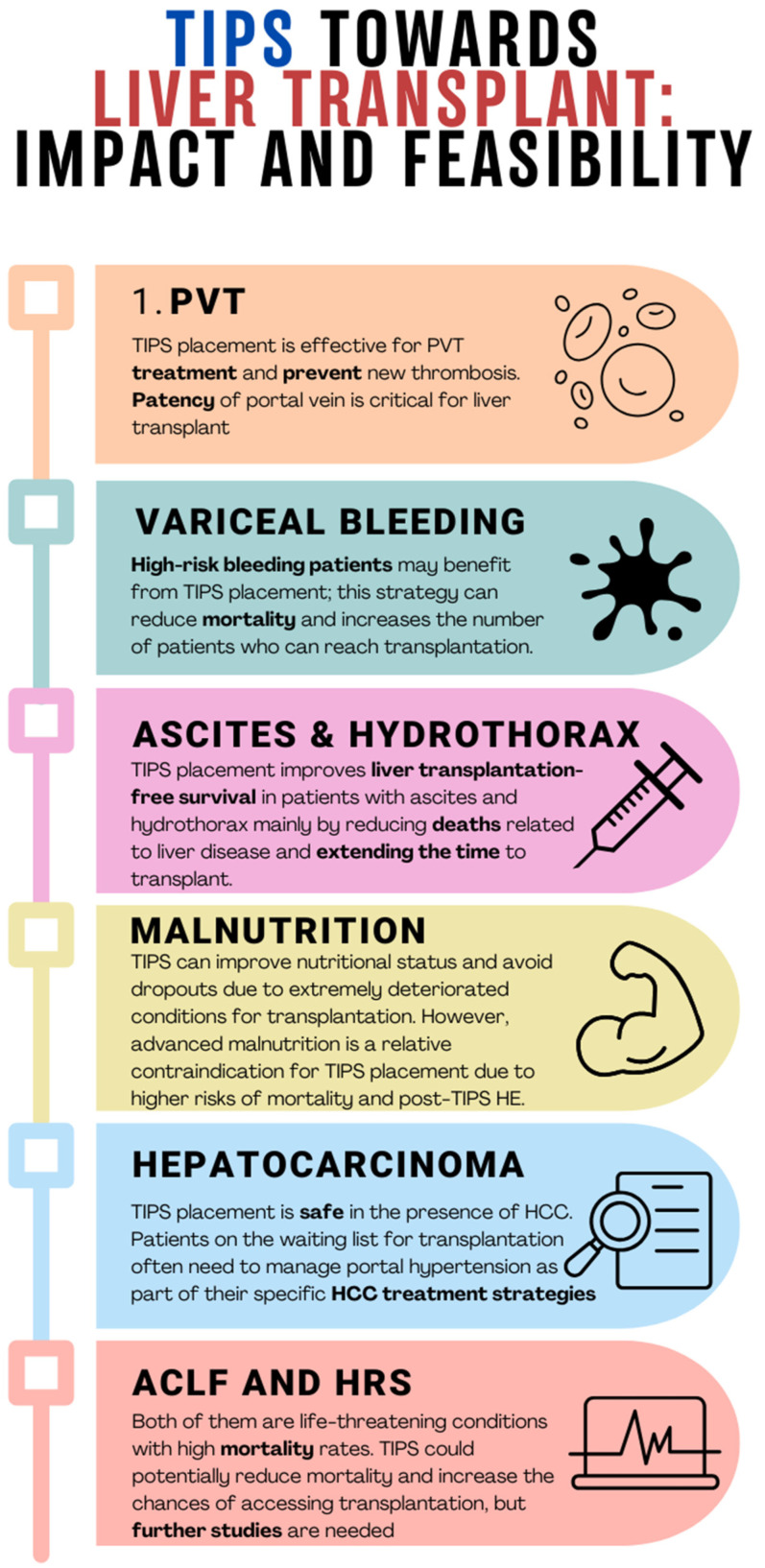
Liver transplantation is currently the only curative therapy for patients with liver cirrhosis. Not all patients in the natural course of the disease will undergo transplantation, but the majority of them will experience portal hypertension and its complications. In addition to medical and endoscopic therapy, a key role in managing these complications is played by the placement of a transjugular intrahepatic portosystemic shunt (TIPS). Some indications for TIPS placement are well-established, and they are expanding and broadening over time. This review aims to describe the role of TIPS in managing patients with liver cirrhosis, in light of liver transplantation. As far as it is known, TIPS placement seems not to affect the surgical aspects of liver transplantation, in terms of intraoperative bleeding rates, postoperative complications, or length of stay in the Intensive Care Unit. However, the placement of a TIPS "towards transplant" can offer advantages in terms of ameliorating a patient's clinical condition at the time of transplantation and improving patient survival. Additionally, the TIPS procedure can help preserve the technical feasibility of the transplant itself. In this context, indications for TIPS placement at an earlier stage are drawing particular attention. However, TIPS insertion in decompensated patients can also lead to serious adverse events. For these reasons, further studies are needed to make reliable recommendations for TIPS in the pre-transplant setting.
Keywords: TIPS; bridge to transplant; liver transplantation; timing; transjugular intrahepatic portosystemic shunt.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
Transjugular intrahepatic portosystemic shunt: Indications, complications, survival and its use as a bridging therapy to liver transplant in Western Australia.J Med Imaging Radiat Oncol. 2017 Aug;61(4):441-447. doi: 10.1111/1754-9485.12563. Epub 2017 Jan 9. J Med Imaging Radiat Oncol. 2017. PMID: 28070962
-
Can pretransplant TIPS be harmful in liver transplantation? A propensity score matching analysis.Surgery. 2020 Jul;168(1):33-39. doi: 10.1016/j.surg.2020.02.017. Epub 2020 Apr 5. Surgery. 2020. PMID: 32268937
-
Operative safety of orthotopic liver transplant in patients with prior transjugular intrahepatic portosystemic shunts: A 20-year experience.Rev Gastroenterol Mex (Engl Ed). 2024 Jan-Mar;89(1):4-10. doi: 10.1016/j.rgmxen.2022.07.005. Epub 2022 Jul 25. Rev Gastroenterol Mex (Engl Ed). 2024. PMID: 35902343 Review.
-
Transjugular Intrahepatic Portosystemic Shunt in Liver Transplant Recipients: Outcomes in Six Adult Patients.Vasc Endovascular Surg. 2023 May;57(4):373-378. doi: 10.1177/15385744221149907. Epub 2023 Jan 2. Vasc Endovascular Surg. 2023. PMID: 36593684
-
Transjugular Intrahepatic Portosystemic Shunt before and after Liver Transplantation.Semin Intervent Radiol. 2014 Sep;31(3):243-7. doi: 10.1055/s-0034-1382791. Semin Intervent Radiol. 2014. PMID: 25177084 Free PMC article. Review.
Cited by
-
Transjugular Intrahepatic Portosystemic Shunt as a Bridge to Abdominal Surgery in Cirrhosis.J Clin Med. 2024 Apr 11;13(8):2213. doi: 10.3390/jcm13082213. J Clin Med. 2024. PMID: 38673486 Free PMC article. Review.
References
-
- [(accessed on 1 December 2023)]. Available online: https://www.who.int/data/gho/data/themes/mortality-and-global-health-est....
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
