

Robotic Hepatectomy plus Biliary Reconstruction for Bismuth Type III and Type IV Hilar Cholangiocarcinoma: State of the Art and Literature Review
- PMID: 38276227
- PMCID: PMC10817587
- DOI: 10.3390/jpm14010012
Robotic Hepatectomy plus Biliary Reconstruction for Bismuth Type III and Type IV Hilar Cholangiocarcinoma: State of the Art and Literature Review
Abstract
Background: In Bismuth type III and IV Hilar Cholangiocarcinoma (III-IV HC), surgical resection is the only chance for long-term survival. As the surgical procedure is complex and Robotic-Assisted Surgery (RAS) may be particularly suitable in this setting, the aim of this study is to evaluate the potential benefits of RAS in III-IV HC in terms of post-operative outcomes.
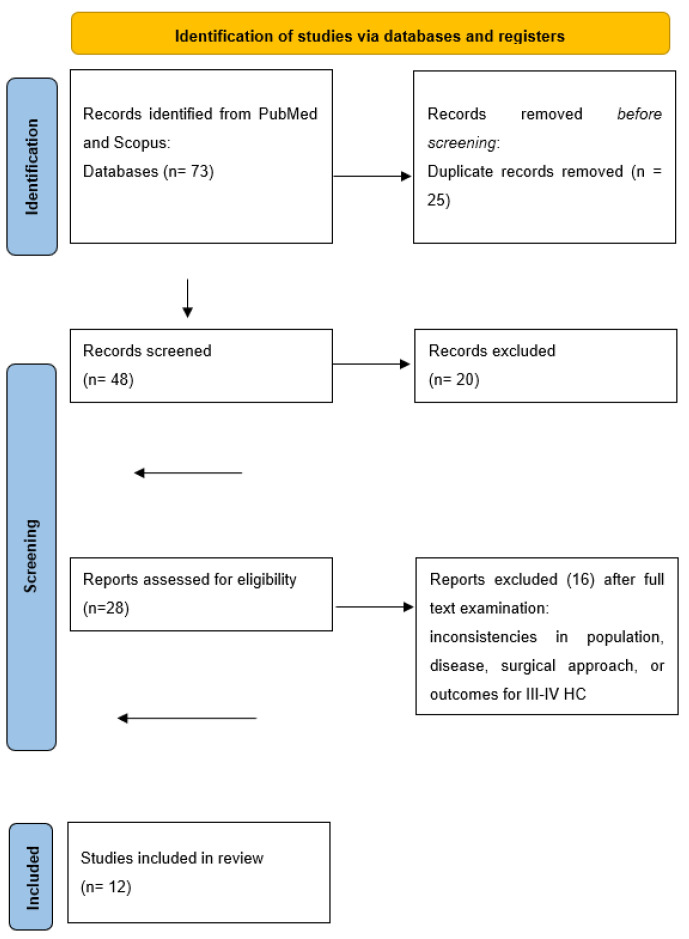
Methods: We conducted a systematic review using the PRISMA checklist for article selection. We searched the PubMed database and included only studies with clinical data about the treatment of III-IV HC using RAS.
Results: A total of 12 papers involving 50 patients were included. All cases were Bismuth IIIa (n = 18), IIIb (n = 27) or IV type (n = 5) and underwent hepatectomy with biliary confluence resection and reconstruction. The mean operative time was 500 minutes with a conversion rate of 4%. The mean hospital stay was 12.2 days, and the morbidity and 30-day mortality rate were 61.9% and 2%, respectively. Over a mean follow up period of 10.1 months, 9/18 cases experienced recurrence (50%).
Conclusions: RAS for III-IV HC is safe and feasible, at least if performed by experienced surgeons on selected cases. The oncological outcomes appear acceptable, given the aggressiveness of this pathology, but further studies are needed to fully elucidate the exact role of robotics in this setting.
Keywords: Hilar Cholangiocarcinoma; da Vinci; robotic liver resection.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
The role of robotic surgery for the treatment of hilar cholangiocarcinoma: A systematic review.Front Oncol. 2022 Sep 28;12:1001838. doi: 10.3389/fonc.2022.1001838. eCollection 2022. Front Oncol. 2022. PMID: 36237328 Free PMC article.
-
Safety and feasibility of laparoscopic radical resection for bismuth types III and IV hilar cholangiocarcinoma: a single-center experience from China.Front Oncol. 2023 Dec 18;13:1280513. doi: 10.3389/fonc.2023.1280513. eCollection 2023. Front Oncol. 2023. PMID: 38188306 Free PMC article.
-
Robotic radical resection for hilar cholangiocarcinoma: perioperative and long-term outcomes of an initial series.Surg Endosc. 2016 Jul;30(7):3060-70. doi: 10.1007/s00464-016-4925-7. Epub 2016 May 18. Surg Endosc. 2016. PMID: 27194255
-
[Partial hepatectomy with skeletonization of the hepatoduodenal ligament for hilar cholangiocarcinoma].Zhonghua Wai Ke Za Zhi. 2004 Feb 22;42(4):210-2. Zhonghua Wai Ke Za Zhi. 2004. PMID: 15062037 Chinese.
-
Robotic hepatectomy and biliary reconstruction for perihilar cholangiocarcinoma: a pioneer western case series.Updates Surg. 2021 Jun;73(3):999-1006. doi: 10.1007/s13304-021-01041-3. Epub 2021 Apr 16. Updates Surg. 2021. PMID: 33861401 Free PMC article. Review.
Cited by
-
Oncologic and cosmetic outcomes of oncoplastic breast-conserving surgery after neoadjuvant systemic therapy: systematic review and meta-analysis.Breast Cancer Res Treat. 2025 Jan;209(2):229-252. doi: 10.1007/s10549-024-07566-6. Epub 2024 Dec 14. Breast Cancer Res Treat. 2025. PMID: 39673644
-
Robotic Revolution in Surgery: Diverse Applications Across Specialties and Future Prospects Review Article.Cureus. 2024 Jan 12;16(1):e52148. doi: 10.7759/cureus.52148. eCollection 2024 Jan. Cureus. 2024. PMID: 38344598 Free PMC article. Review.
-
"Hepatic hilum area priority, liver posterior first": An optimized strategy in laparoscopic resection for type III-IV hilar cholangiocarcinoma.World J Gastrointest Surg. 2024 Jul 27;16(7):2167-2174. doi: 10.4240/wjgs.v16.i7.2167. World J Gastrointest Surg. 2024. PMID: 39087123 Free PMC article.
References
-
- Banales J.M., Marin J.G., Lamarca A., Rodrigues P.M., Khan S.A., Roberts L.R., Cardinale V., Carpino G., Andersen J.B., Braconi C., et al. Cholangiocarcinoma 2020: The next horizon in mechanisms and management. Nat. Rev. Gastroenterol. Hepatol. 2020;17:557. doi: 10.1038/s41575-020-0310-z. - DOI - PMC - PubMed
-
- Van Keulen A.M., Franssen S.S., van derGeest L.G., De Boer M.T., Coenraad M., van Driel L.M.J.W., Erdmann J.I., Haj Mohammad N., Heij L., Klümpen H.J., et al. Nationwide treatment and outcomes of perihilar cholangiocarcinoma. Liver Int. 2021;41:1945–1953. doi: 10.1111/liv.14856. - DOI - PMC - PubMed
-
- Morelli L., Di Franco G., Guadagni S., Rossi L., Palmeri M., Furbetta N., Gianardi D., Bianchini M., Caprili G., D’Isidoro C., et al. Robot-assisted total mesorectal excision for rectal cancer: Case-matched comparison of short-term surgical and functional outcomes between the da Vinci Xi and Si. Surg. Endosc. 2018;32:589–600. doi: 10.1007/s00464-017-5708-5. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
