

Tumor- and circulating-free DNA methylation identifies clinically relevant small cell lung cancer subtypes
- PMID: 38278149
- PMCID: PMC10982990
- DOI: 10.1016/j.ccell.2024.01.001
Tumor- and circulating-free DNA methylation identifies clinically relevant small cell lung cancer subtypes
Abstract
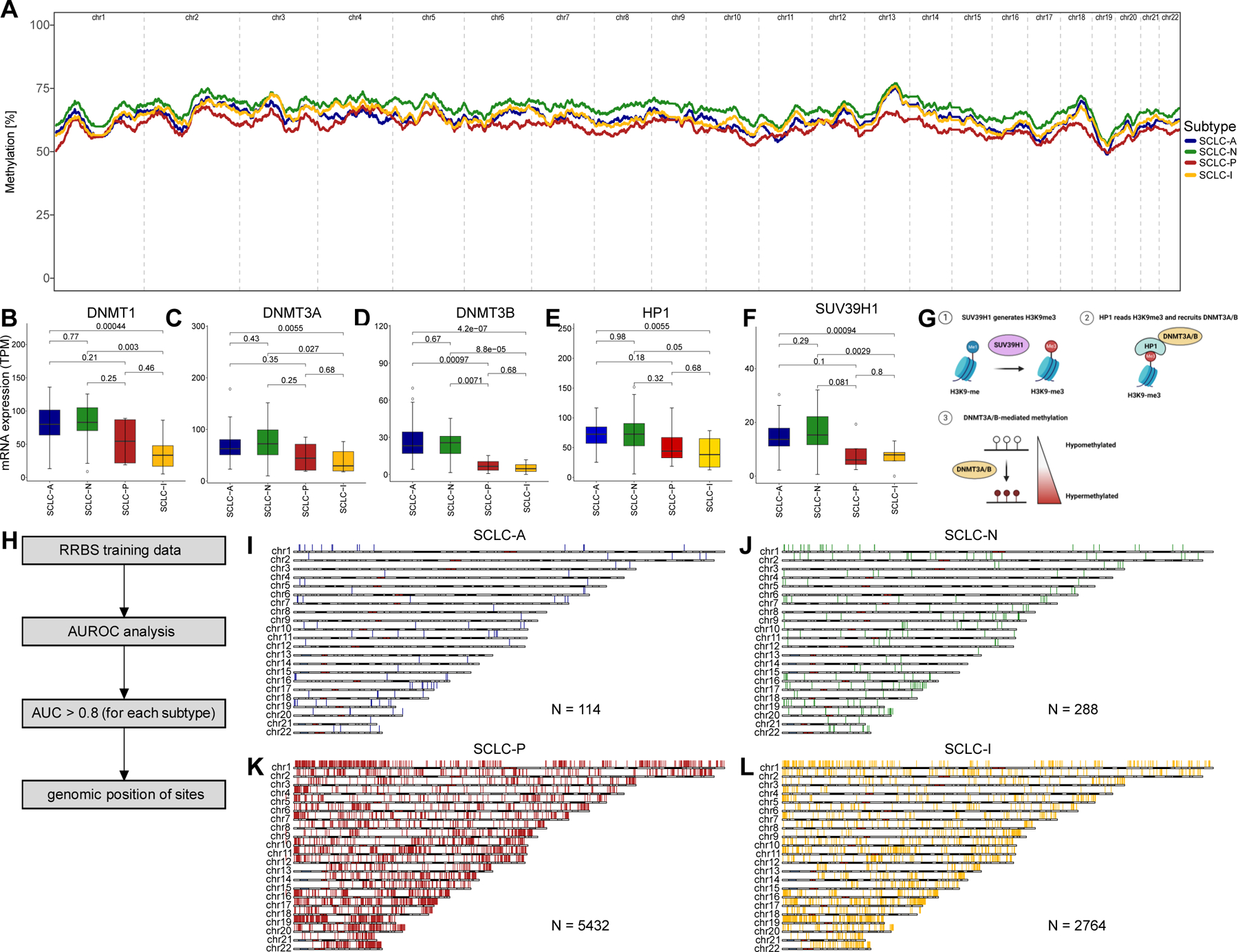
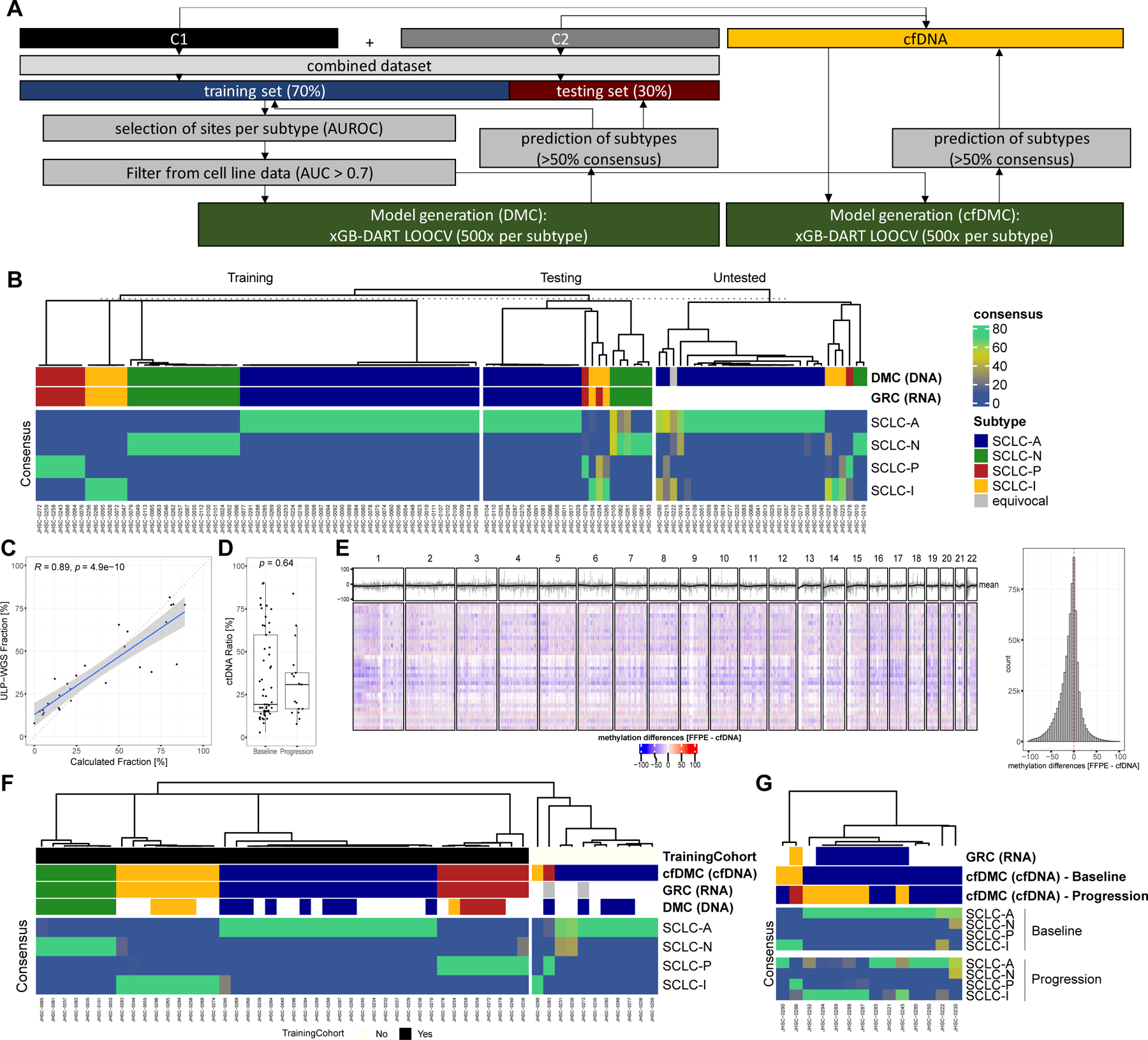
Small cell lung cancer (SCLC) is an aggressive malignancy composed of distinct transcriptional subtypes, but implementing subtyping in the clinic has remained challenging, particularly due to limited tissue availability. Given the known epigenetic regulation of critical SCLC transcriptional programs, we hypothesized that subtype-specific patterns of DNA methylation could be detected in tumor or blood from SCLC patients. Using genomic-wide reduced-representation bisulfite sequencing (RRBS) in two cohorts totaling 179 SCLC patients and using machine learning approaches, we report a highly accurate DNA methylation-based classifier (SCLC-DMC) that can distinguish SCLC subtypes. We further adjust the classifier for circulating-free DNA (cfDNA) to subtype SCLC from plasma. Using the cfDNA classifier (cfDMC), we demonstrate that SCLC phenotypes can evolve during disease progression, highlighting the need for longitudinal tracking of SCLC during clinical treatment. These data establish that tumor and cfDNA methylation can be used to identify SCLC subtypes and might guide precision SCLC therapy.
Keywords: DNA methylation; SCLC; biomarker; cfDNA; ctDNA; epigenetics; gene expression; liquid biopsy; lung cancer; subtyping.
Copyright © 2024 The Authors. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of interests S.H., C.M.G., L.A.B., and J.V.H. own intellectual property on the classification of SCLC from DNA methylation and gene expression. D.F., A.W., A.S., and C.A.S. are full time employees of Nucleix and own stocks and stock options of Nucleix. Furthermore, S.H. reports consulting fees from Guardant Health, AstraZeneca, Boehringer Ingelheim, and Qiagen. C.M.G. is a member of the advisory board at Jazz Pharmaceuticals, AstraZeneca, and Bristol Myers Squibb and served as speaker for AstraZeneca and BeiGene. P.R. received travel support from AstraZeneca, BMS, and MSD. E.A. reports consulting fees from Eli Lilly, AstraZeneca, BMS, Boehringer Ingelheim, Takeda, Roche, and MSD, speaker’s fees from AstraZeneca, BMS, Boehringer Ingelheim, Roche, and MSD, research funding from Roche and AstraZeneca and travel support from AstraZeneca and Takeda. P.H. reports research grants from Thermo Fisher Scientific and Biocartis, and speakers’ fees from AstraZeneca, Roche, Novartis, Bristol-Myers Squibb, Pfizer, Bayer, Illumina, Biocartis, Thermo Fisher Scientific, AbbVie, Amgen, Janssen, Eli Lilly, Daiichi Sankyo, Pierre Fabre, and Guardant. V.H. reports speakers’ fees from BMS. C.M.L. reports personal fees from Amgen, Arrivent, AstraZeneca, Blueprints Medicine, Cepheid, D2G Oncology, Daiichi Sankyo, Eli Lilly, EMD Serono, Foundation Medicine, Genentech, Janssen, Medscape, Novartis, Pfizer, Puma, Syros, and Takeda. N.V. receives consulting fees from Sanofi, Regeneron, Oncocyte, and Eli Lilly, and research funding from Mirati. M.B.N. receives royalties and licensing fees from Spectrum Pharmaceuticals. I.H. received personal as well as institutional funding from Nucleix. J.Z. served on advisory board for AstraZeneca and Geneplus and received speaker’s fees from BMS, Geneplus, OrigMed, Innovent and grants from Merck, Johnson and Johnson. L.A.B received consulting fees and research funding from AstraZeneca, GenMab, Sierra Oncology, research funding from ToleroPharmaceuticals and served as advisor or consultant for PharmaMar, AbbVie, Bristol-Myers Squibb, Alethia, Merck, Pfizer, Jazz Pharmaceuticals, Genentech, and Debiopharm Group. J.V.H. served as advisor for AstraZeneca, EMD Serono, Boehringer-Ingelheim, Catalyst, Genentech, GlaxoSmithKline, Guardant Health, Foundation medicine, Hengrui Therapeutics, Eli Lilly, Novartis, Spectrum, Sanofi, Takeda, Mirati Therapeutics, BMS, BrightPath Biotherapeutics, Janssen Global Services, Nexus Health Systems, Pneuma Respiratory, Kairos Venture Investments, Roche, Leads Biolabs, RefleXion, Chugai Pharmaceuticals, received research support from AstraZeneca, GlaxoSmithKline, Spectrum as well as royalties and licensing fees from Spectrum.
Figures


References
-
- Paz-Ares L, Dvorkin M, Chen Y, Reinmuth N, Hotta K, Trukhin D, Statsenko G, Hochmair MJ, Ozguroglu M, Ji JH, et al. (2019). Durvalumab plus platinum-etoposide versus platinum-etoposide in first-line treatment of extensive-stage small-cell lung cancer (CASPIAN): a randomised, controlled, open-label, phase 3 trial. Lancet 394, 1929–1939. 10.1016/S0140-6736(19)32222-6. - DOI - PubMed
-
- Paz-Ares L, Champiat S, Lai WV, Izumi H, Govindan R, Boyer M, Hummel HD, Borghaei H, Johnson ML, Steeghs N, et al. (2023). Tarlatamab, a First-In-Class DLL3-Targeted Bispecific T-Cell Engager, in Recurrent Small Cell Lung Cancer: An Open-Label, Phase I Study. J Clin Oncol, JCO2202823. 10.1200/JCO.22.02823. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- U01 CA213273/CA/NCI NIH HHS/United States
- U54 CA217450/CA/NCI NIH HHS/United States
- U24 CA213274/CA/NCI NIH HHS/United States
- CC2008/WT_/Wellcome Trust/United Kingdom
- UG1 CA233259/CA/NCI NIH HHS/United States
- R50 CA243698/CA/NCI NIH HHS/United States
- R50 CA265307/CA/NCI NIH HHS/United States
- R01 CA207295/CA/NCI NIH HHS/United States
- P50 CA070907/CA/NCI NIH HHS/United States
- CC2008/MRC_/Medical Research Council/United Kingdom
- R01 CA276178/CA/NCI NIH HHS/United States
- U01 CA224276/CA/NCI NIH HHS/United States
- U01 CA256780/CA/NCI NIH HHS/United States
- P30 CA016672/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
