

Evaluating the efficacy and safety of pozelimab in patients with CD55 deficiency with hyperactivation of complement, angiopathic thrombosis, and protein-losing enteropathy disease: an open-label phase 2 and 3 study
- PMID: 38278170
- PMCID: PMC10979753
- DOI: 10.1016/S0140-6736(23)02358-9
Evaluating the efficacy and safety of pozelimab in patients with CD55 deficiency with hyperactivation of complement, angiopathic thrombosis, and protein-losing enteropathy disease: an open-label phase 2 and 3 study
Abstract
Background: CD55 deficiency with hyperactivation of complement, angiopathic thrombosis, and protein-losing enteropathy (CHAPLE) is an ultra-rare genetic disorder characterised by intestinal lymphatic damage, lymphangiectasia, and protein-losing enteropathy caused by overactivation of the complement system. We assessed the efficacy and safety of pozelimab, an antibody blocking complement component 5.
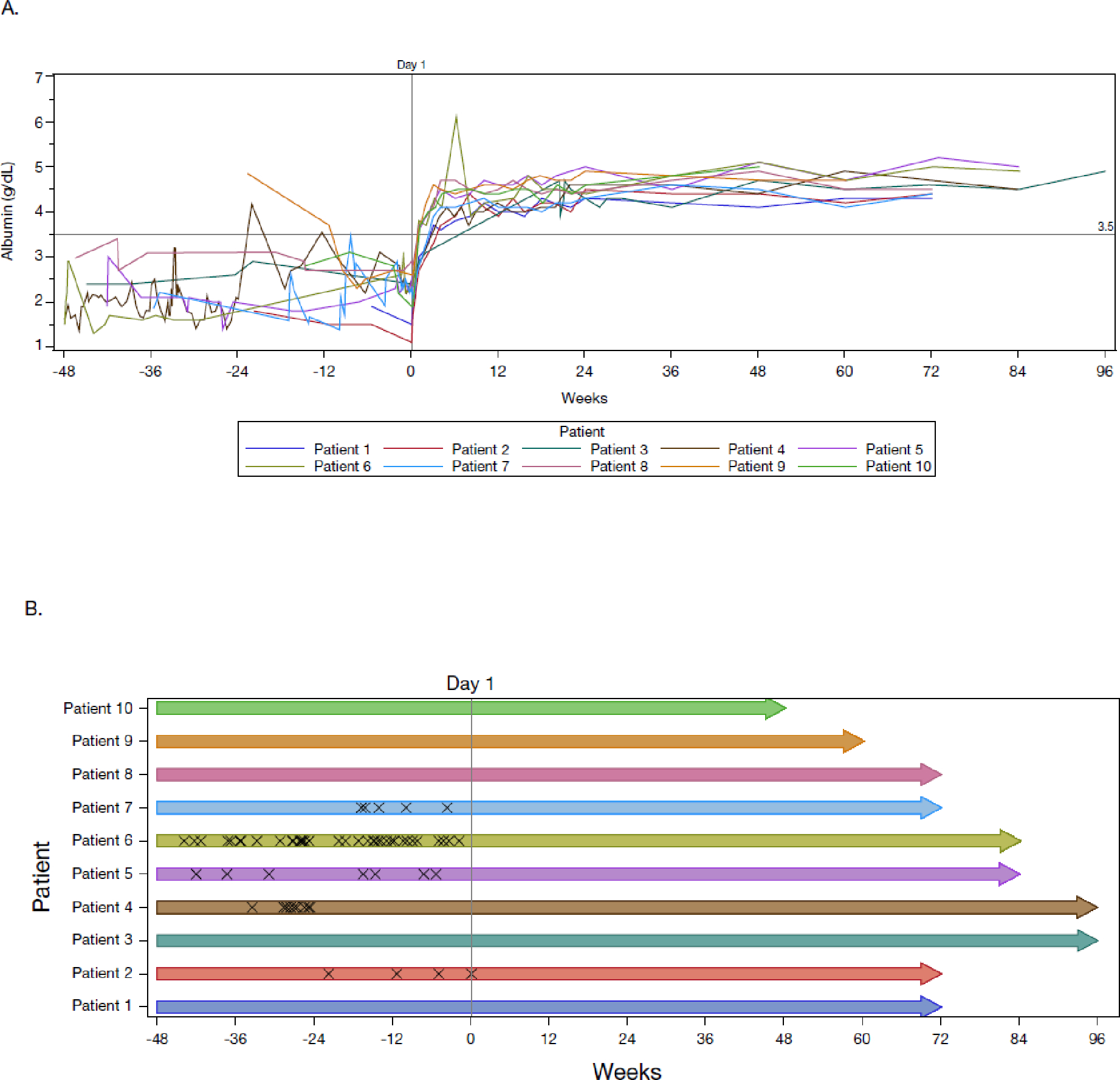
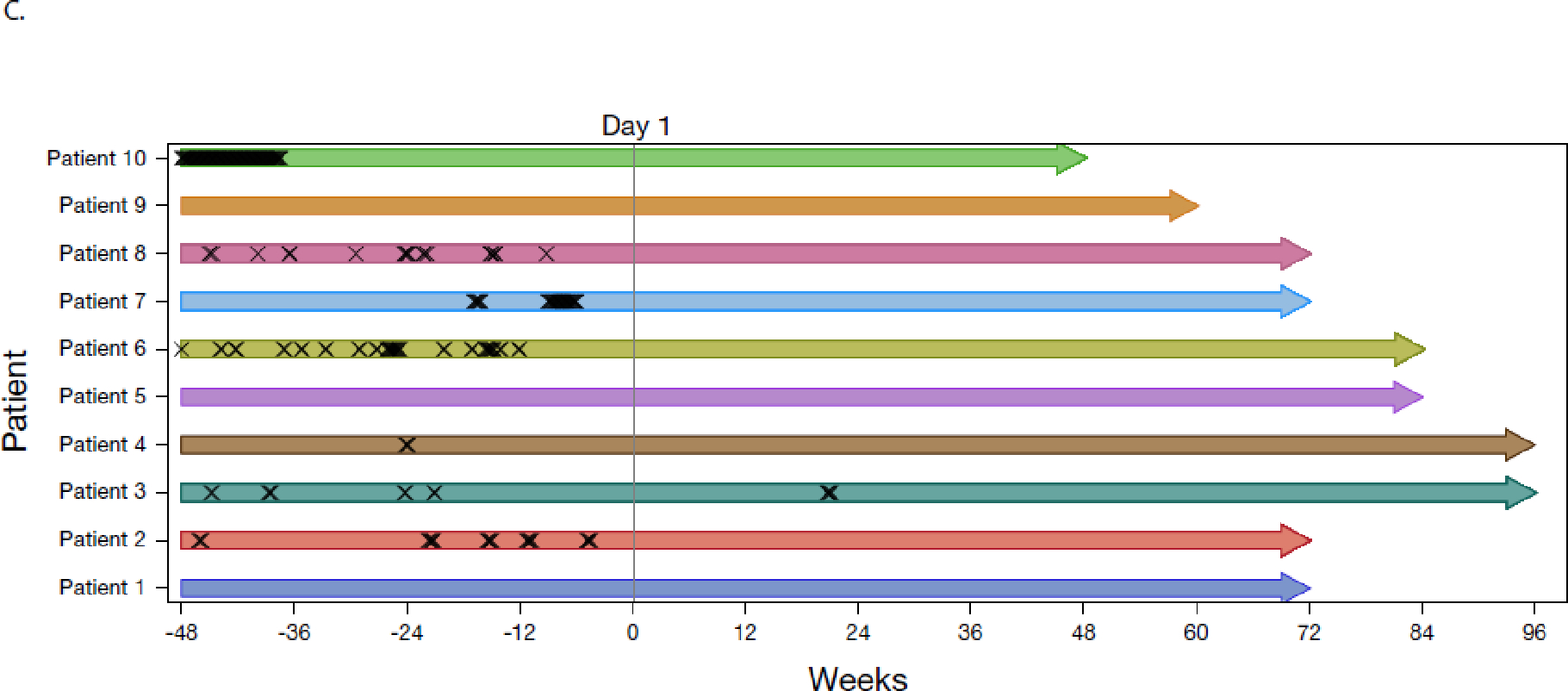
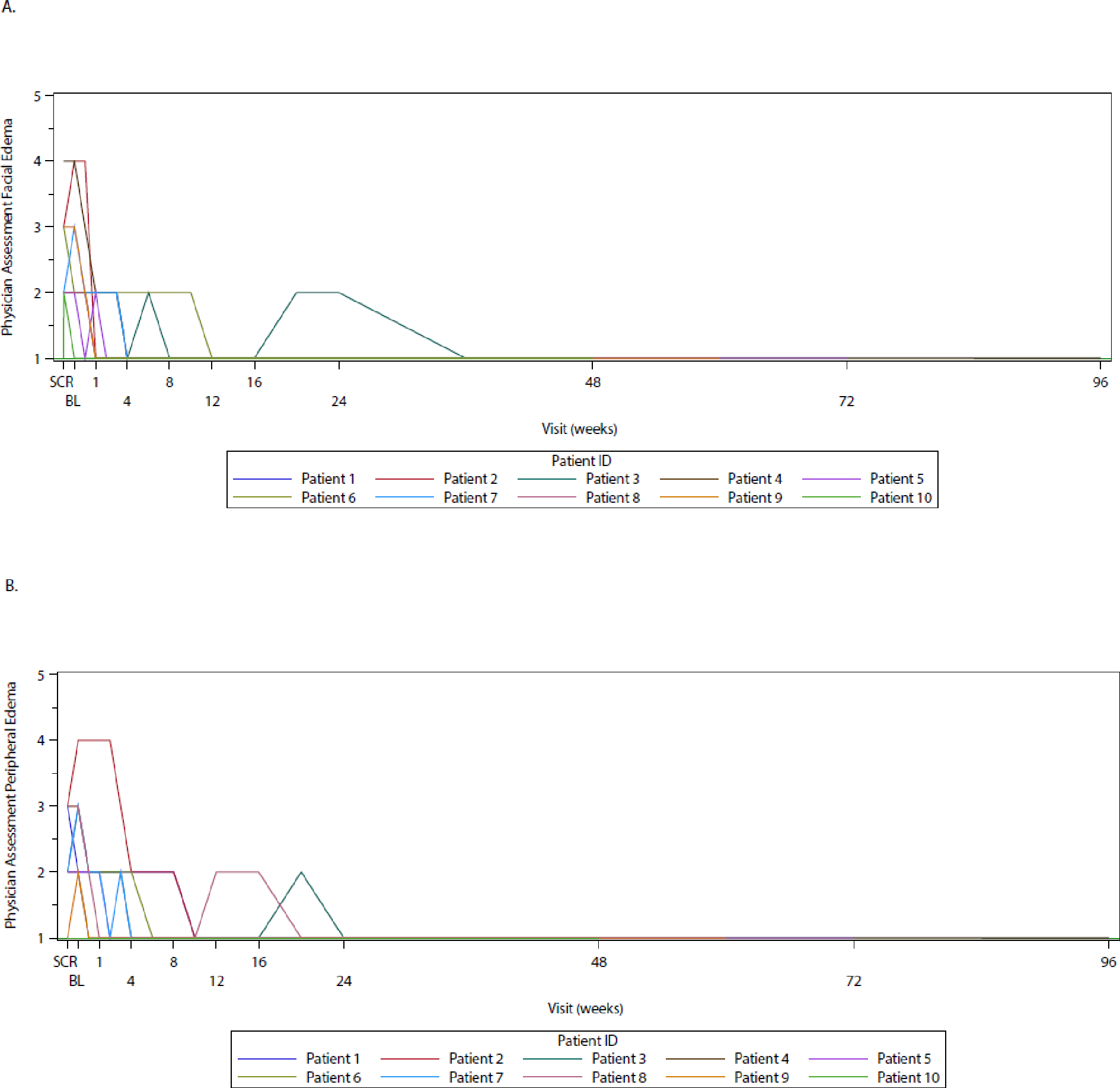
Methods: This open-label, single-arm, historically controlled, multicentre phase 2 and 3 study evaluated ten patients with CHAPLE disease. This study was conducted at three hospitals in Thailand, Türkiye, and the USA. Patients aged 1 year or older with a clinical diagnosis of CHAPLE disease and a CD55 loss-of-function variant identified by genetic analysis and confirmed by flow cytometry or western blot of CD55 from peripheral blood cells were eligible for this study. Patients received a single intravenous loading dose of pozelimab 30 mg per kg of bodyweight, followed by a once-per-week subcutaneous dose over the treatment period based on bodyweight at a concentration of 200 mg/mL as either a single injection (<40 kg bodyweight) or two injections (≥40 kg bodyweight). The primary endpoint was proportion of patients with serum albumin normalisation with an improvement in active clinical outcomes and no worsening in inactive clinical outcomes (frequency of problematic abdominal pain, bowel movement frequency, facial oedema severity, and peripheral oedema severity) at week 24 compared with baseline, assessed in the full analysis set. This study is registered with ClinicalTrials.gov (NCT04209634) and is active but not recruiting.
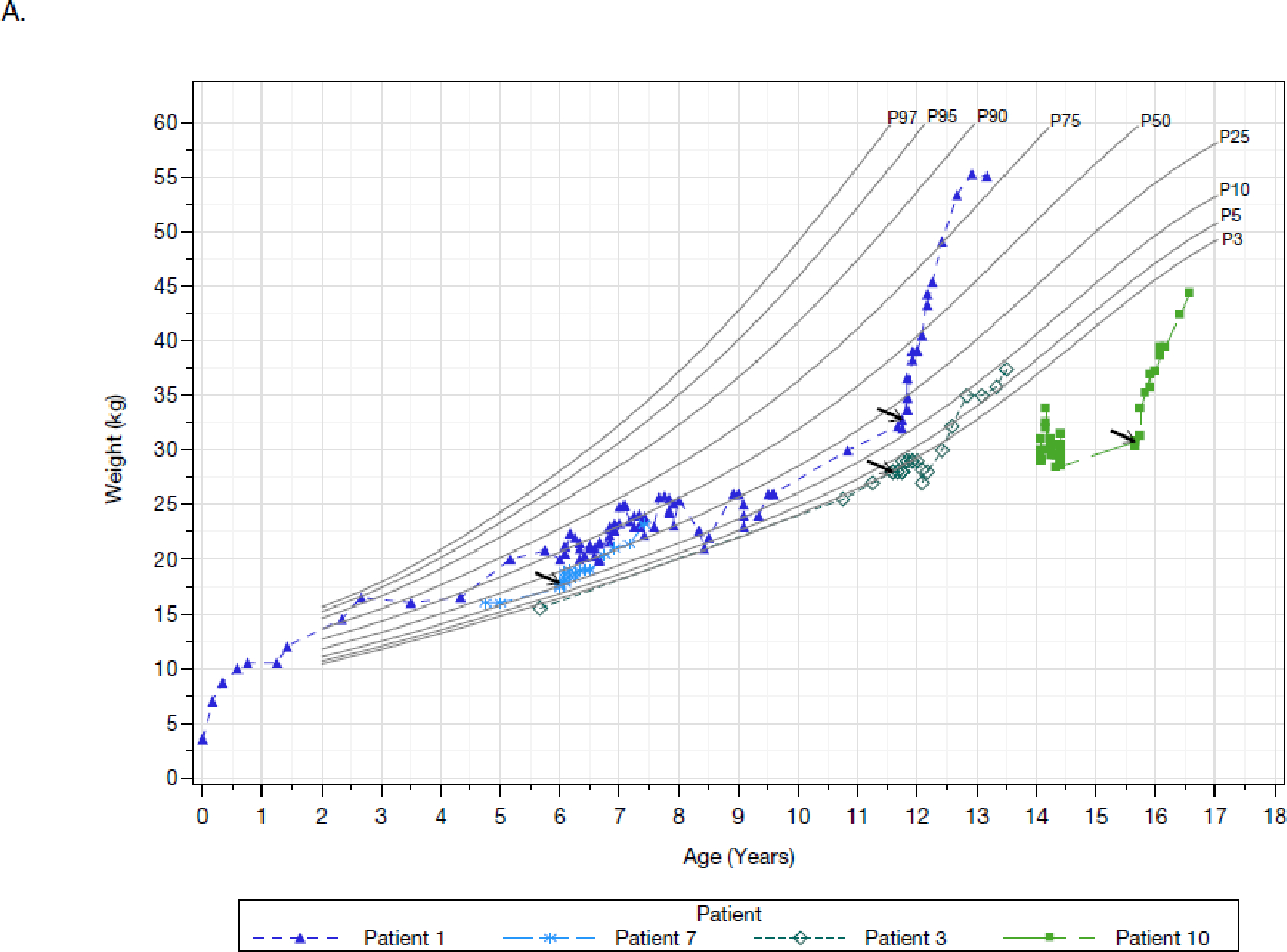
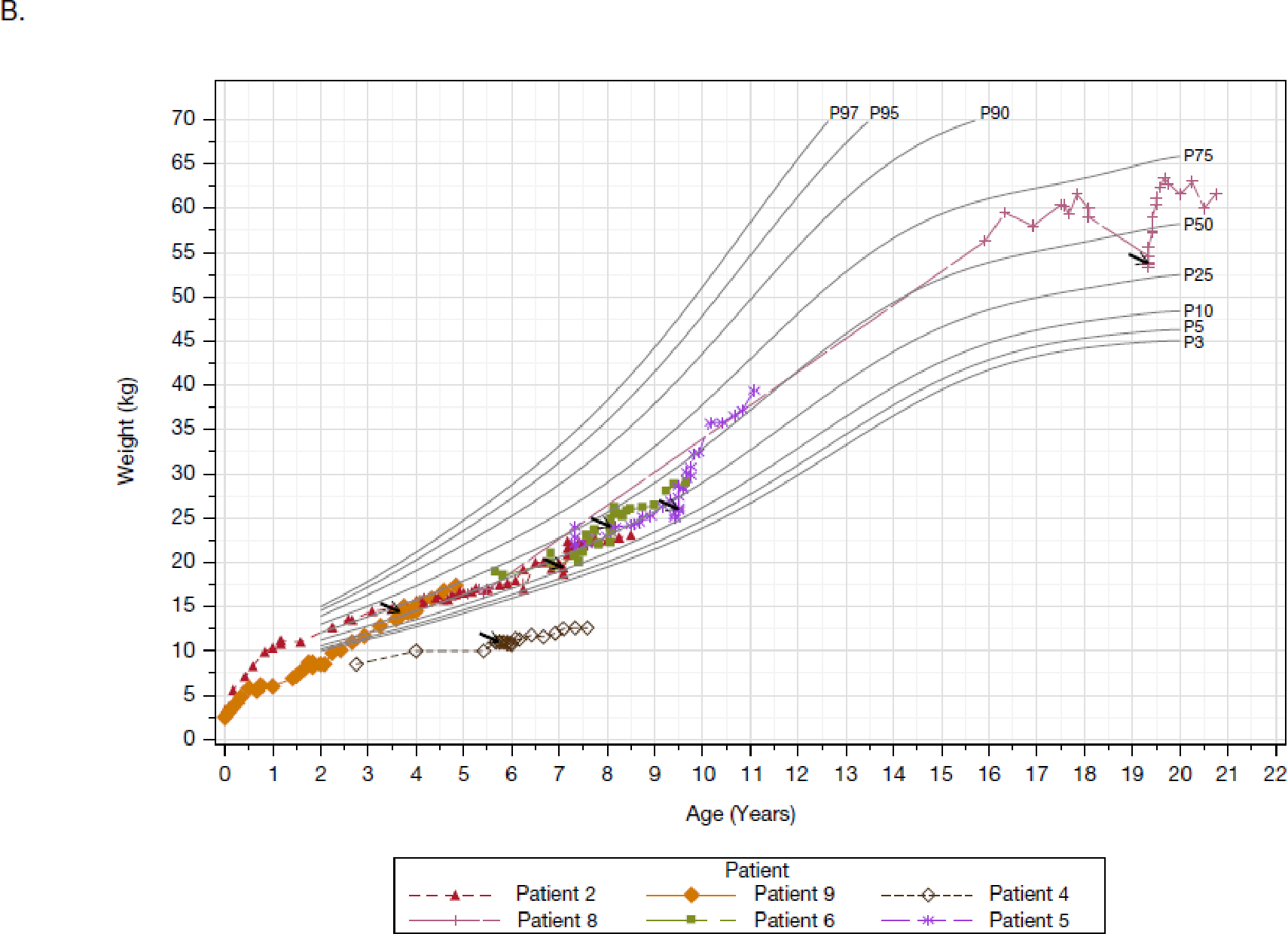
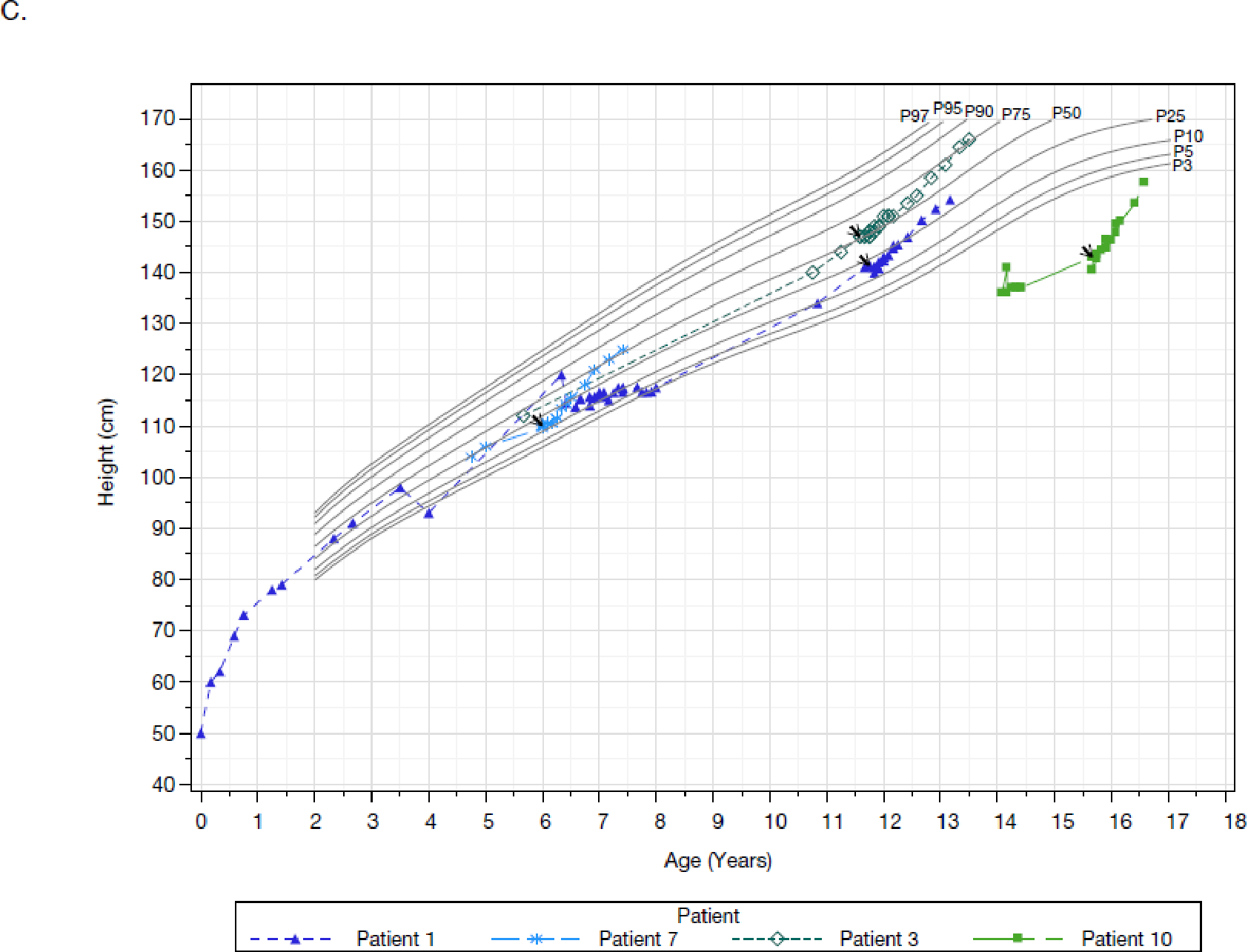
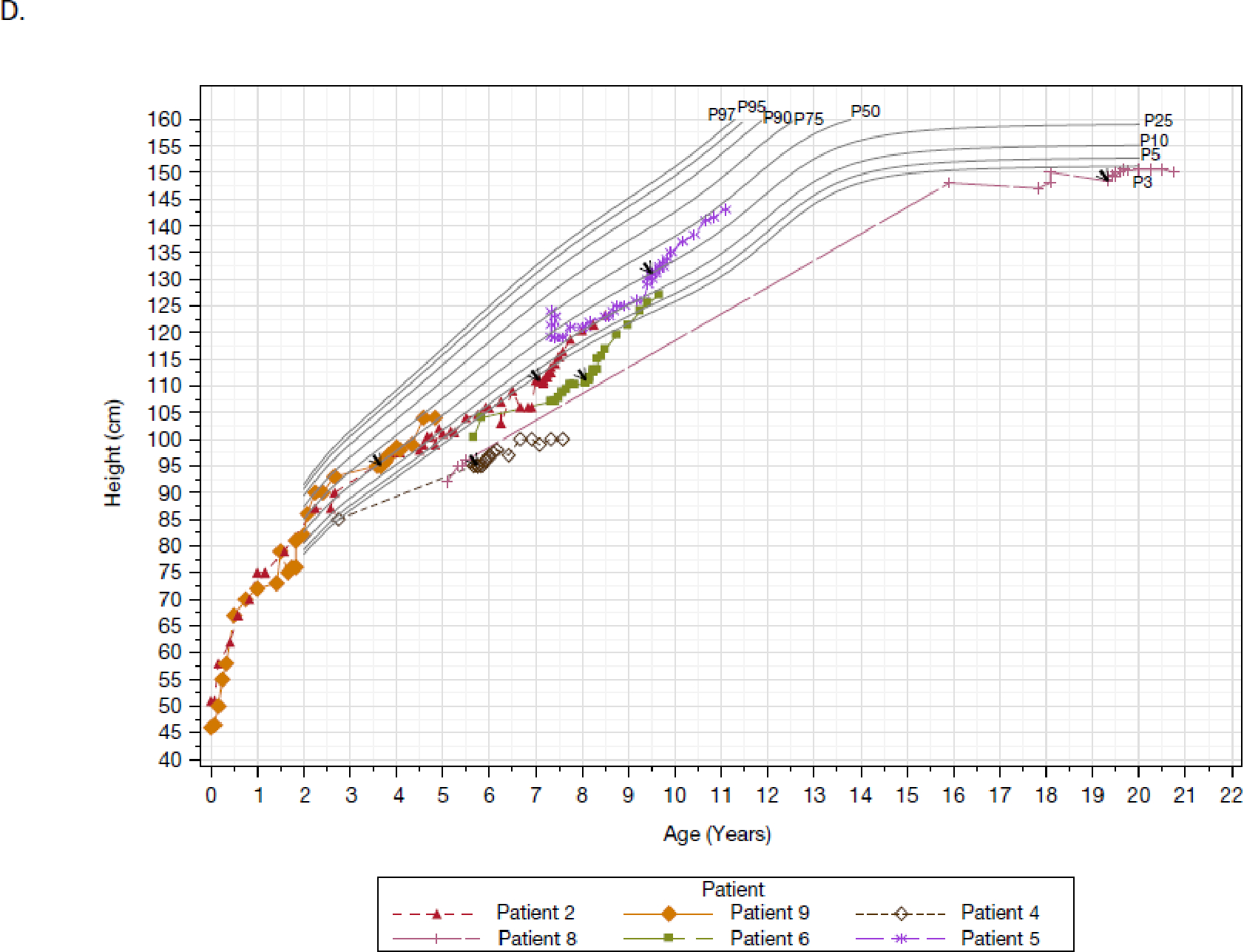
Findings: 11 patients were recruited between Jan 27, 2020, and May 12, 2021, ten of which were enrolled in the study and included in the analysis populations. The efficacy data corresponded to all patients completing the week 48 assessment and having at least 52 weeks of treatment exposure, and the safety data included an additional 90 days of follow-up and corresponded to all patients having at least 72 weeks of treatment. Patients were predominantly paediatric (with a median age of 8·5 years), and originated from Türkiye, Syria, Thailand, and Bolivia. Patients had markedly low weight-for-age and stature-for-age at baseline, and mean albumin at baseline was 2·2 g/dL, which was considerably less than the local laboratory reference range. After pozelimab treatment, all ten patients had serum albumin normalisation and improvement with no worsening in clinical outcomes. There was a complete inhibition of the total complement activity. Nine patients had adverse events; two were severe events, and one patient had an adverse event considered related to pozelimab.
Interpretation: Pozelimab inhibits complement overactivation and resolves the clinical and laboratory manifestations of CHAPLE disease. Pozelimab is the only currently approved therapeutic drug for patients with this life-threatening, ultra-rare condition. In patients with protein-losing enteropathy where known causes have been excluded, testing for a CD55 deficiency should be contemplated. A diagnosis of CHAPLE disease should lead to early consideration of treatment with pozelimab.
Funding: Regeneron Pharmaceuticals and the Division of Intramural Research, National Institute of Allergy and Infectious Diseases, National Institutes of Health.
Copyright © 2024 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declaration of interests AO is a consultant and steering committee member for Regeneron Pharmaceuticals; received sample analysis support for a previous collaborative study (https://doi.org/10.1038/s41590-020-00830-z) from Regeneron Pharmaceuticals; and has a pending patent on component 5 inhibitor treatment in CHAPLE disease. VC, NS, and KS received support to conduct the study and received provision of the investigational product from Regeneron Pharmaceuticals. JJJ, TB, and LP are Regeneron Pharmaceuticals employees and stockholders. KAM is a Regeneron Pharmaceuticals employee and stockholder and has both pending and issued patents with Regeneron Pharmaceuticals. HBF is a consultant and advisory board member for Regeneron Pharmaceuticals. IJF is an associate on a cooperative research and development agreement between Merck Pharmaceuticals and the National Institutes for Health. OAH and GDY are Regeneron Pharmaceuticals employees and stockholders and have a pending patent on complement component 5 inhibitor treatment in CHAPLE disease. MJL received support for a federally approved cooperative research and development agreement to support the clinical trial and has a pending patent on complement component 5 inhibitor treatment in CHAPLE disease. All other authors declare no competing interests.
Figures
Comment in
-
A new drug for rare diseases: pozelimab for CHAPLE disease.Lancet. 2024 Feb 17;403(10427):592-593. doi: 10.1016/S0140-6736(23)02652-1. Epub 2024 Jan 23. Lancet. 2024. PMID: 38278169 No abstract available.
References
-
- Lublin DM, Atkinson JP. Decay-accelerating factor: biochemistry, molecular biology, and function. Annu Rev Immunol. 1989;7:35–58. - PubMed
-
- Kurolap A, Eshach-Adiv O, Hershkovitz T, Paperna T, Mory A, Oz-Levi D, et al. Loss of CD55 in Eculizumab-Responsive Protein-Losing Enteropathy. N Engl J Med. 2017;377(1):87–9. - PubMed
-
- Hagin D, Lahav D, Freund T, Shamai S, Brazowski E, Fishman S, et al. Eculizumab-Responsive Adult Onset Protein Losing Enteropathy, Caused by Germline CD55-Deficiency and Complicated by Aggressive Angiosarcoma. J Clin Immunol. 2021;41(2):477–81. - PubMed
-
- Soliris. Soliris [package insert]. Boston, MA: Alexion Pharmaceuticals, Inc.; 2020. 2020.
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
