

Sepsis mimics among presumed sepsis patients at intensive care admission: a retrospective observational study
- PMID: 38280062
- PMCID: PMC11636973
- DOI: 10.1007/s15010-023-02158-w
Sepsis mimics among presumed sepsis patients at intensive care admission: a retrospective observational study
Abstract
Background: Diagnosing sepsis remains a challenge because of the lack of gold-standard diagnostics. Since there are no simple, broadly accepted criteria for infection, there is a risk of misclassifying sepsis patients (sepsis mimics) among patients with organ failure. The main objective of this study was to investigate the proportion of non-infected patients (sepsis mimics) in ICU patients with presumed sepsis at intensive care unit (ICU) admission.
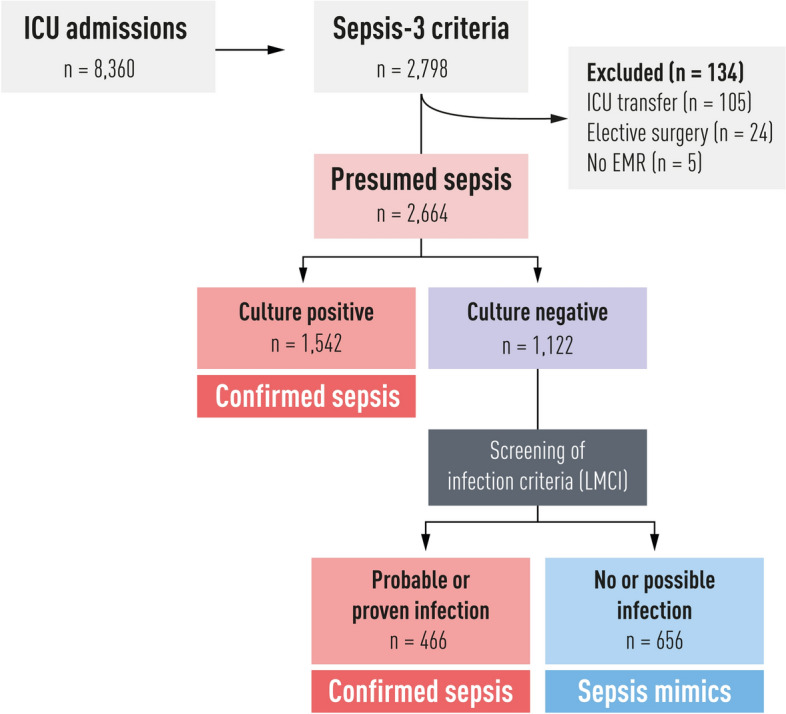
Methods: Adult patients were screened retrospectively during 3.5 years in four ICUs in Sweden for fulfilment of the sepsis-3 criteria at ICU admission (presumed sepsis). Proxy criteria for suspected infection were sampled blood culture(s) and concomitant antibiotic administration. Culture-negative presumed sepsis patients were screened for infection according to the Linder-Mellhammar Criteria of Infection (LMCI). Sepsis mimics were defined as without probable infection according to the LMCI. Confirmed sepsis was defined as presumed sepsis after the exclusion of sepsis mimics.
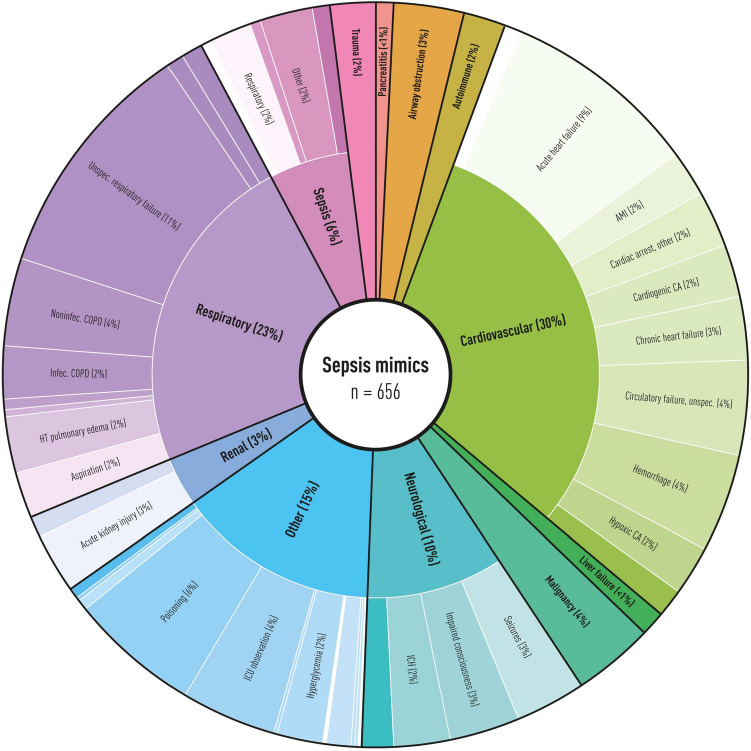
Results: In the ICU presumed sepsis cohort (2664 patients), 25% were considered sepsis mimics. The most common reasons for ICU admission among sepsis mimics were acute heart failure and unspecific respiratory failure. Comparing sepsis mimics and confirmed sepsis showed that confirmed sepsis patients were slightly more severely ill but had similar mortality. C-reactive protein had modest discriminatory power (AUROC 0.71) with confirmed sepsis as the outcome.
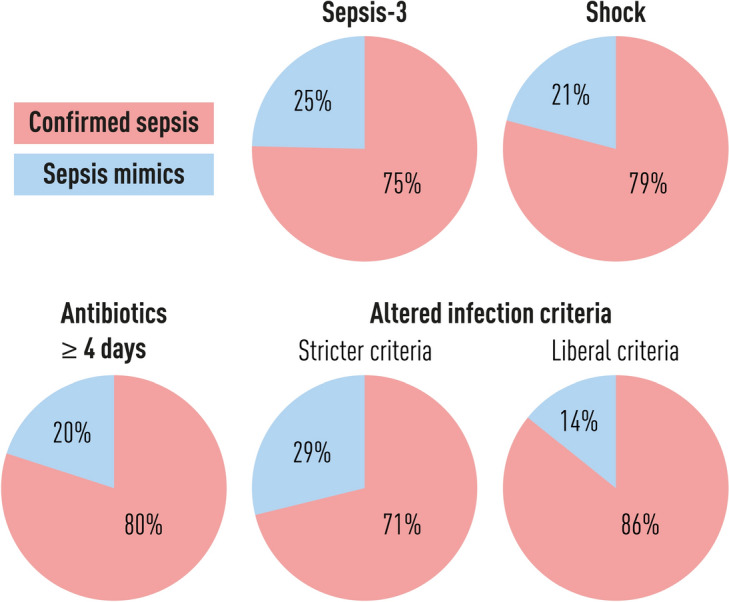
Conclusions: One-fourth of a presumed ICU sepsis population identified with the sepsis-3 criteria could be considered sepsis mimics. The high proportion of sepsis mimics has a potential dilutional effect on the presumed sepsis population, which threatens the validity of results from sepsis studies using recommended sepsis criteria.
Keywords: Biomarkers; C-reactive protein; Critical care; Infections; Leukocytes; Sepsis; Septic; Shock.
© 2024. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
Publication types
MeSH terms
Grants and funding
- 2021-0907/Regional research support, Region Skåne
- 2022-1284/Regional research support, Region Skåne
- 2022:YF0009, 2022-0075/Governmental funding of clinical research within the Swedish National Health Service (ALF)
- 2022-0352, 2022-0458/Swedish Heart and Lund Foundation (HLF)
- 2021-0833/Crafoord Foundation
LinkOut - more resources
Full Text Sources
Medical
Research Materials
