

Hypertension and urologic chronic pelvic pain syndrome: An analysis of MAPP-I data
- PMID: 38281923
- PMCID: PMC10822153
- DOI: 10.1186/s12894-024-01407-w
Hypertension and urologic chronic pelvic pain syndrome: An analysis of MAPP-I data
Abstract
Background: Urologic chronic pelvic pain syndrome (UCPPS), which includes interstitial cystitis/bladder pain syndrome (IC/BPS) and chronic prostatitis (CP/CPPS), is associated with increased voiding frequency, nocturia, and chronic pelvic pain. The cause of these diseases is unknown and likely involves many different mechanisms. Dysregulated renin-angiotensin-aldosterone-system (RAAS) signaling is a potential pathologic mechanism for IC/BPS and CP/CPPS. Many angiotensin receptor downstream signaling factors, including oxidative stress, fibrosis, mast cell recruitment, and increased inflammatory mediators, are present in the bladders of IC/BPS patients and prostates of CP/CPPS patients. Therefore, we aimed to test the hypothesis that UCPPS patients have dysregulated angiotensin signaling, resulting in increased hypertension compared to controls. Secondly, we evaluated symptom severity in patients with and without hypertension and antihypertensive medication use.
Methods: Data from UCPPS patients (n = 424), fibromyalgia or irritable bowel syndrome (positive controls, n = 200), and healthy controls (n = 415) were obtained from the NIDDK Multidisciplinary Approach to the Study of Chronic Pelvic Pain I (MAPP-I). Diagnosis of hypertension, current antihypertensive medications, pain severity, and urinary symptom severity were analyzed using chi-square test and t-test.
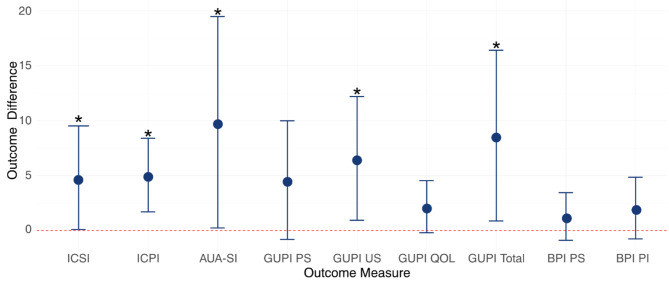
Results: The combination of diagnosis and antihypertensive medications use was highest in the UCPPS group (n = 74, 18%), followed by positive (n = 34, 17%) and healthy controls (n = 48, 12%, p = 0.04). There were no differences in symptom severity based on hypertension in UCPPS and CP/CPPS; however, IC/BPS had worse ICSI (p = 0.031), AUA-SI (p = 0.04), and BPI pain severity (0.02). Patients (n = 7) with a hypertension diagnosis not on antihypertensive medications reported the greatest severity of pain and urinary symptoms.
Conclusion: This pattern of findings suggests that there may be a relationship between hypertension and UCPPS. Treating hypertension among these patients may result in reduced pain and symptom severity. Further investigation on the relationship between hypertension, antihypertensive medication use, and UCPPS and the role of angiotensin signaling in UCPPS conditions is needed.
Keywords: Angiotensin; Chronic prostatitis; Hypertension; Interstitial cystitis/bladder pain syndrome; MAPP; Urologic chronic pelvic pain syndrome.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- Bartoletti R, Cai T, Mondaini N, Dinelli N, Pinzi N, Pavone C, Gontero P, Gavazzi A, Giubilei G, Prezioso D, et al. Prevalence, incidence estimation, risk factors and characterization of chronic prostatitis/chronic pelvic pain syndrome in urological hospital outpatients in Italy: results of a multicenter case-control observational study. J Urol. 2007;178(6):2411–5. doi: 10.1016/j.juro.2007.08.046. - DOI - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
