

Single-cell analysis of immune and stroma cell remodeling in clear cell renal cell carcinoma primary tumors and bone metastatic lesions
- PMID: 38281962
- PMCID: PMC10823713
- DOI: 10.1186/s13073-023-01272-6
Single-cell analysis of immune and stroma cell remodeling in clear cell renal cell carcinoma primary tumors and bone metastatic lesions
Abstract
Background: Despite therapeutic advances, once a cancer has metastasized to the bone, it represents a highly morbid and lethal disease. One third of patients with advanced clear cell renal cell carcinoma (ccRCC) present with bone metastasis at the time of diagnosis. However, the bone metastatic niche in humans, including the immune and stromal microenvironments, has not been well-defined, hindering progress towards identification of therapeutic targets.
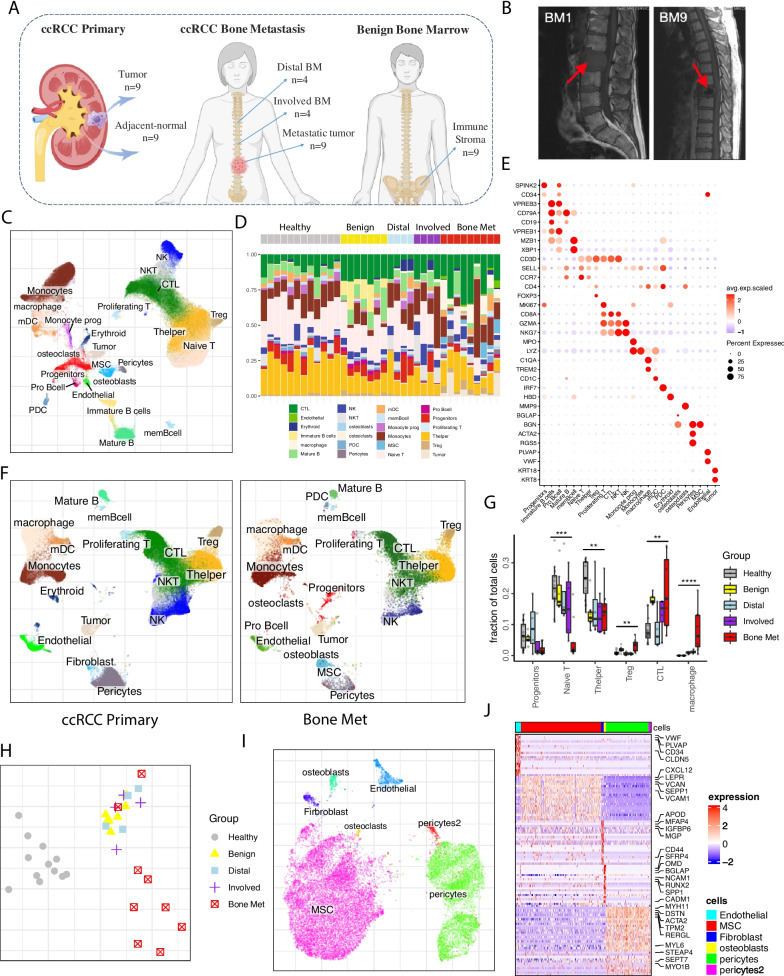
Methods: We collected fresh patient samples and performed single-cell transcriptomic profiling of solid metastatic tissue (Bone Met), liquid bone marrow at the vertebral level of spinal cord compression (Involved), and liquid bone marrow from a different vertebral body distant from the tumor site but within the surgical field (Distal), as well as bone marrow from patients undergoing hip replacement surgery (Benign). In addition, we incorporated single-cell data from primary ccRCC tumors (ccRCC Primary) for comparative analysis.
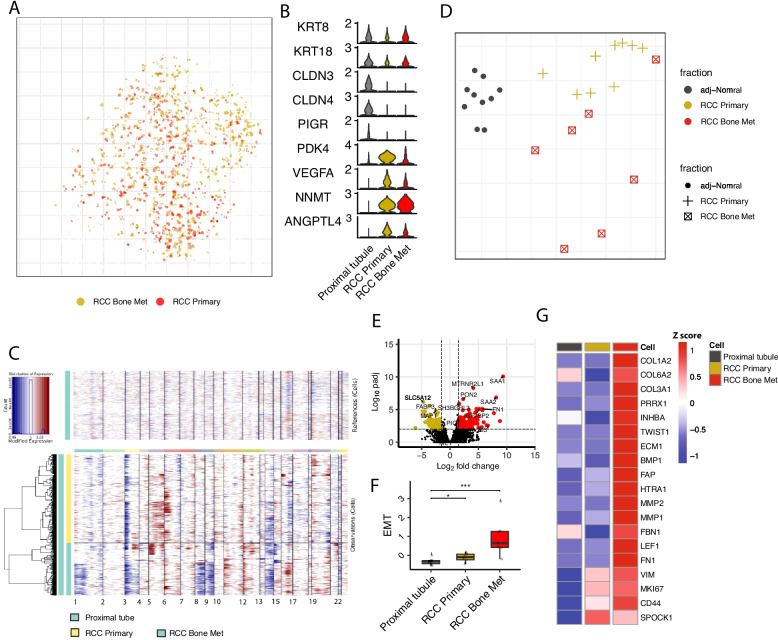
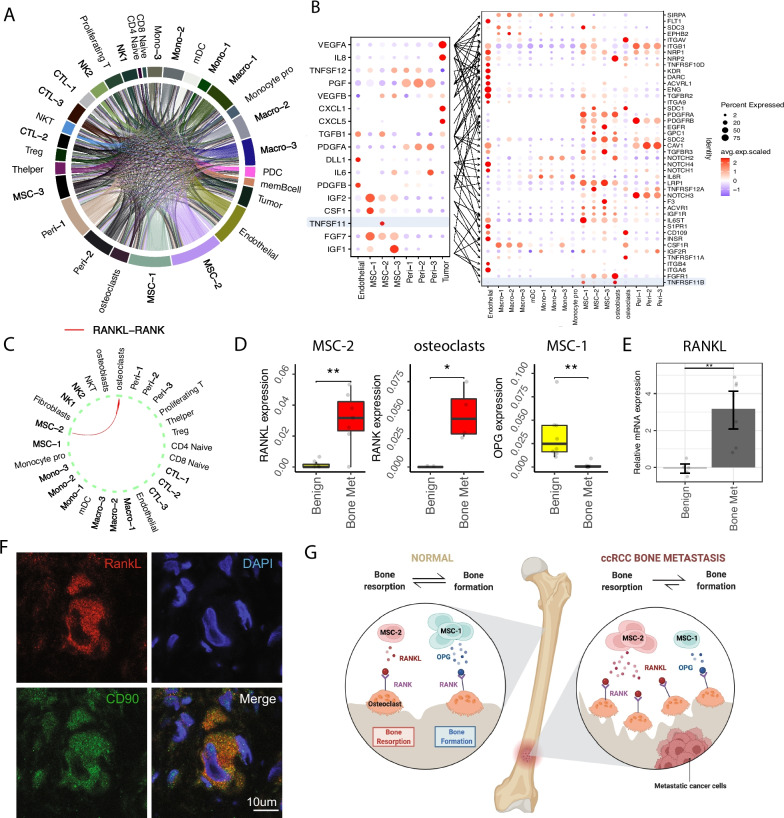
Results: The bone marrow of metastatic patients is immune-suppressive, featuring increased, exhausted CD8 + cytotoxic T cells, T regulatory cells, and tumor-associated macrophages (TAM) with distinct transcriptional states in metastatic lesions. Bone marrow stroma from tumor samples demonstrated a tumor-associated mesenchymal stromal cell population (TA-MSC) that appears to be supportive of epithelial-to mesenchymal transition (EMT), bone remodeling, and a cancer-associated fibroblast (CAFs) phenotype. This stromal subset is associated with poor progression-free and overall survival and also markedly upregulates bone remodeling through the dysregulation of RANK/RANKL/OPG signaling activity in bone cells, ultimately leading to bone resorption.
Conclusions: These results provide a comprehensive analysis of the bone marrow niche in the setting of human metastatic cancer and highlight potential therapeutic targets for both cell populations and communication channels.
© 2023. The Author(s).
Conflict of interest statement
P.V.K serves on the Scientific Advisory Board to Celsius Therapeutics, Inc., and Biomage Inc. D.B.S. is a co-founder and holds equity in Clear Creek Bio and is a consultant and holds equity in SAFI Biosolutions. D.T.S. is a founder, director, and stockholder of Magenta Therapeutics, Clear Creek Bio, and LifeVaultBio. He is a director and stockholder of Agios Pharmaceuticals and Editas Medicines and a founder and stockholder of Fate Therapeutics and Geruda Therapeutics. He is a consultant for FOG Pharma, Inzen Therapeutics, ResoluteBio, and VCanBio and receives sponsored research support on an unrelated project from Sumitomo Dianippon. D.B.S. is a founder, consultant, and shareholder for Clear Creek Bio. The remaining authors declare that they do not have any competing interests.
Figures



References
-
- Macedo F, Ladeira K, Pinho F, Saraiva N, Bonito N, Pinto L, et al. Bone metastases: an overview. Oncol Rev. 2016;11:321. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5444408/. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
Research Materials
Miscellaneous
