Evolution of spontaneous portosystemic shunts over time and following aetiological intervention in patients with cirrhosis
- PMID: 38283756
- PMCID: PMC10820312
- DOI: 10.1016/j.jhepr.2023.100977
Evolution of spontaneous portosystemic shunts over time and following aetiological intervention in patients with cirrhosis
Abstract
Background & aims: Spontaneous portosystemic shunts (SPSS) develop frequently in cirrhosis. Changes over time and the effect of aetiological interventions on SPSS are unknown, so we aimed to explore the effect of these variables on SPSS evolution.
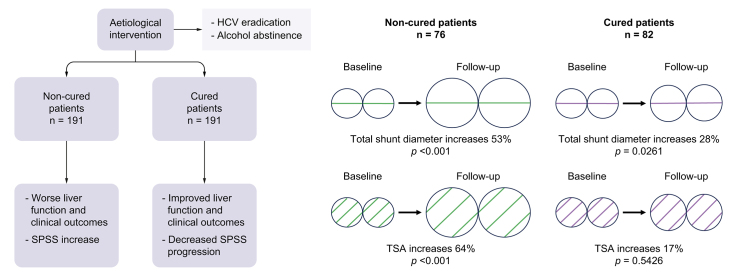
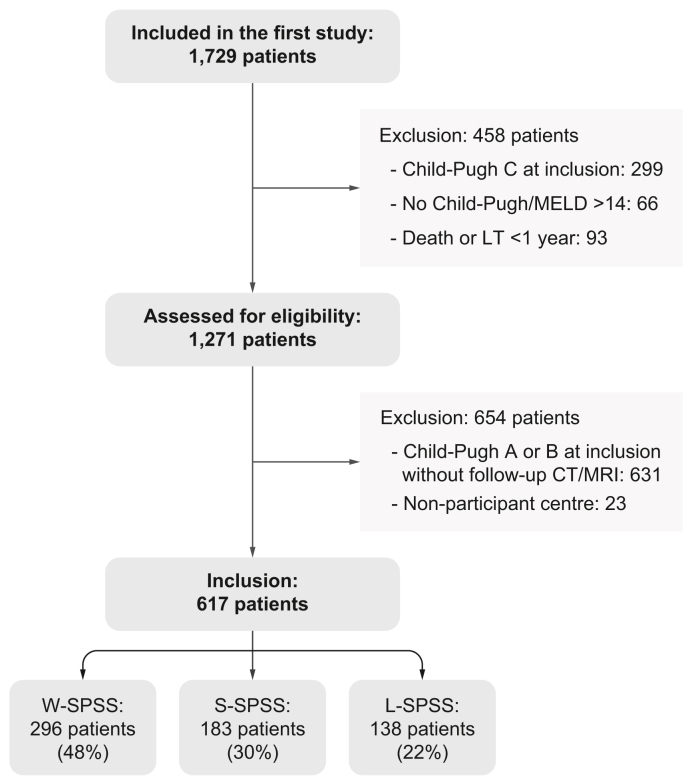
Methods: Patients with cirrhosis from the Baveno VI-SPSS cohort were selected provided a follow-up abdominal CT or MRI scan was available. Clinical and laboratory data were collected at baseline and follow-up. Imaging tests were reviewed to evaluate changes in the presence and size of SPSS (large (L)-SPSS was ≥8 mm) over time. Regarding alcohol- or HCV-related cirrhosis, two populations were defined: cured patients (abstinent from alcohol or successful HCV therapy), and non-cured patients.
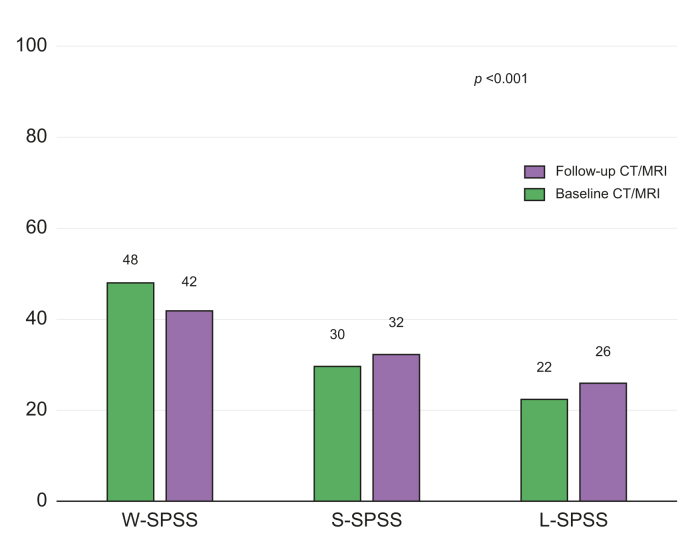
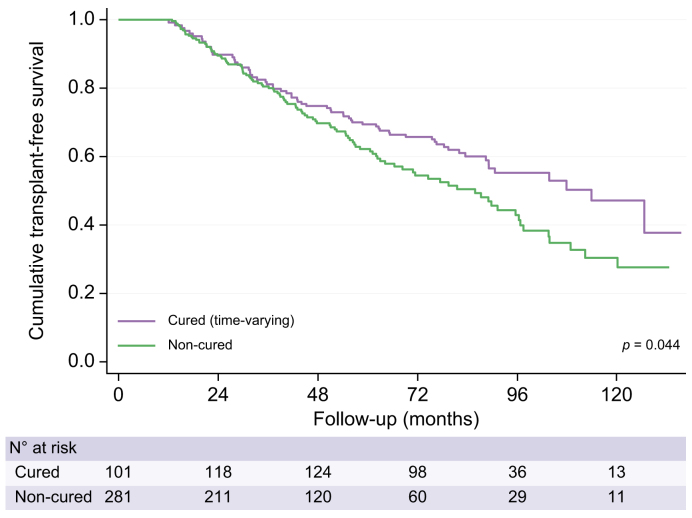
Results: A total of 617 patients were included. At baseline SPSS distribution was 22% L-SPSS, 30% small (S)-SPSS, and 48% without (W)-SPSS. During follow-up (median follow-up of 63 months), SPSS distribution worsened: L-SPSS 26%, S-SPSS 32%, and W-SPSS 42% (p <0.001). Patients with worse liver function during follow-up showed a simultaneous aggravation in SPSS distribution. Non-cured patients (n = 191) experienced a significant worsening in liver function, more episodes of liver decompensation and lower transplant-free survival compared to cured patients (n = 191). However, no differences were observed regarding SPSS distribution at inclusion and at follow-up, with both groups showing a trend to worsening. Total shunt diameter increased more in non-cured (52%) than in cured patients (28%). However, total shunt area (TSA) significantly increased only in non-cured patients (74 to 122 mm2, p <0.001).
Conclusions: The presence of SPSS in cirrhosis increases over time and parallels liver function deterioration. Aetiological intervention in these patients reduces liver-related complications, but SPSS persist although progression is decreased.
Impact and implications: There is no information regarding the evolution of spontaneous portosystemic shunts (SPSS) during the course of cirrhosis, and especially after disease regression with aetiological interventions, such as HCV treatment with direct-acting antivirals or alcohol abstinence. These results are relevant for clinicians dealing with patients with cirrhosis and portal hypertension because they have important implications for the management of cirrhosis with SPSS after disease regression. From a practical point of view, physicians should be aware that in advanced cirrhosis with portal hypertension, after aetiological intervention, SPSS mostly persist despite liver function improvement, and complications related to SPSS may still develop.
Keywords: Advanced chronic liver disease; Alcohol; Ascites; Collateral vessels; Computed tomography; Hepatic encephalopathy; Hepatitis C virus; Magnetic resonance imaging; Portal hypertension; Sustained virological response.
© 2023 The Authors.
Conflict of interest statement
JG has received consulting fees from Boehringer Ingelheim and speaking fees from Echosens. MS-T has received consulting fees from Grifols. AK has served as speaker for Novo Nordisk, Norgine, Siemens and Nordic Bioscience and participated in advisory boards for Norgine, Siemens, Resalis Therapeutics, Boehringer Ingelheim and Novo Nordisk, all outside the submitted work. Research support Norgine, Siemens, Nordic Bioscience, Astra, Echosense. Consulting Takeda, Resalis Therapeutics, Zealand Pharma, Novo Nordisk, Boehringer Ingelheim. Board member and co-founder Evido. Please refer to the accompanying ICMJE disclosure forms for further details.
Figures