

Iatrogenic Alzheimer's disease in recipients of cadaveric pituitary-derived growth hormone
- PMID: 38287166
- PMCID: PMC10878974
- DOI: 10.1038/s41591-023-02729-2
Iatrogenic Alzheimer's disease in recipients of cadaveric pituitary-derived growth hormone
Abstract
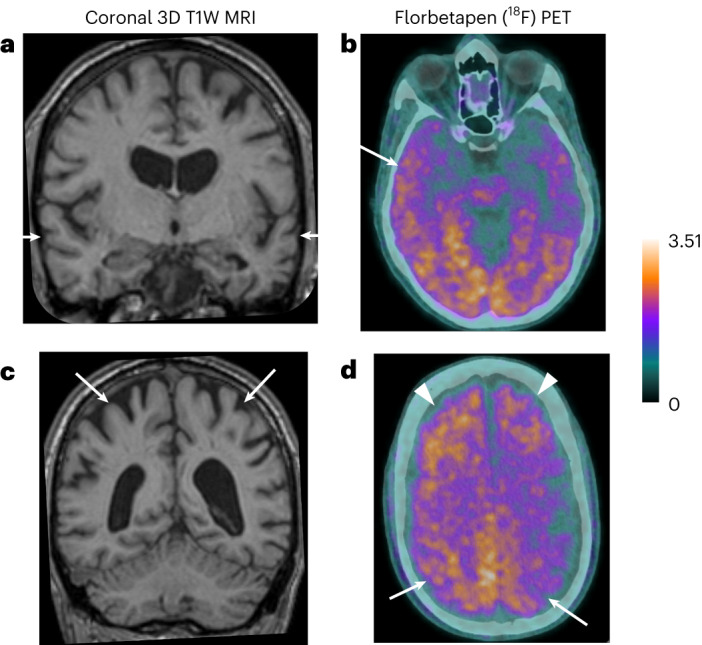
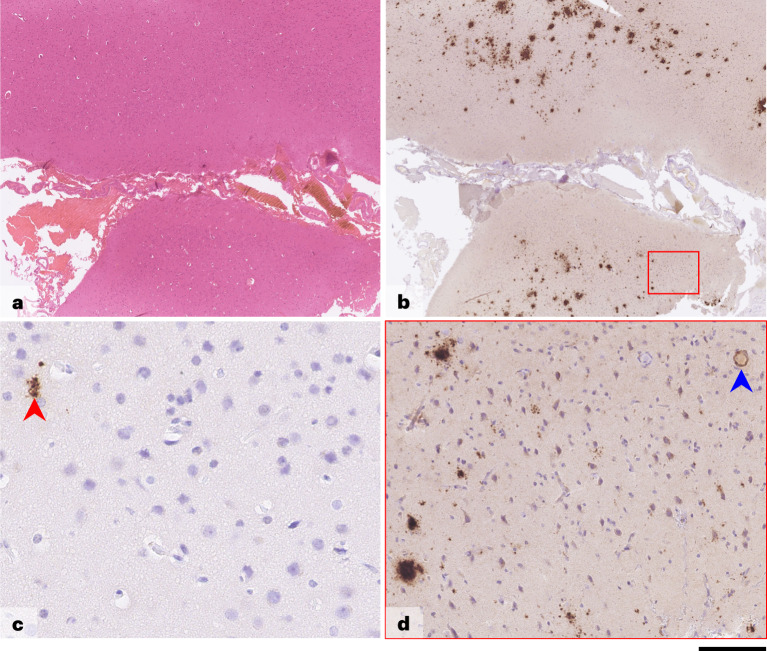
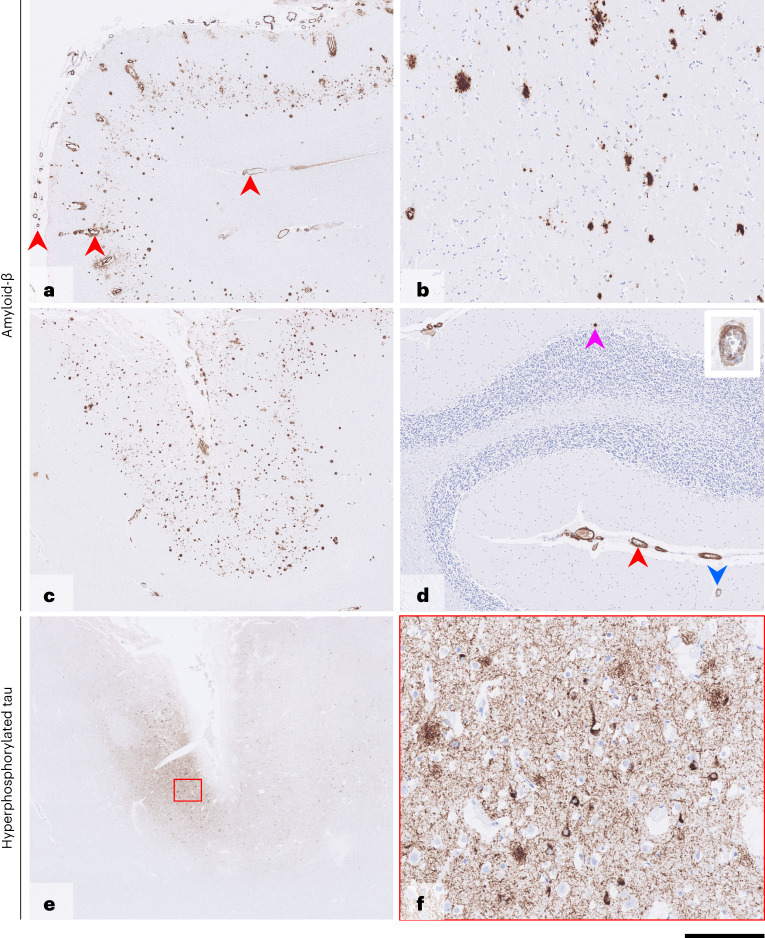
Alzheimer's disease (AD) is characterized pathologically by amyloid-beta (Aβ) deposition in brain parenchyma and blood vessels (as cerebral amyloid angiopathy (CAA)) and by neurofibrillary tangles of hyperphosphorylated tau. Compelling genetic and biomarker evidence supports Aβ as the root cause of AD. We previously reported human transmission of Aβ pathology and CAA in relatively young adults who had died of iatrogenic Creutzfeldt-Jakob disease (iCJD) after childhood treatment with cadaver-derived pituitary growth hormone (c-hGH) contaminated with both CJD prions and Aβ seeds. This raised the possibility that c-hGH recipients who did not die from iCJD may eventually develop AD. Here we describe recipients who developed dementia and biomarker changes within the phenotypic spectrum of AD, suggesting that AD, like CJD, has environmentally acquired (iatrogenic) forms as well as late-onset sporadic and early-onset inherited forms. Although iatrogenic AD may be rare, and there is no suggestion that Aβ can be transmitted between individuals in activities of daily life, its recognition emphasizes the need to review measures to prevent accidental transmissions via other medical and surgical procedures. As propagating Aβ assemblies may exhibit structural diversity akin to conventional prions, it is possible that therapeutic strategies targeting disease-related assemblies may lead to selection of minor components and development of resistance.
© 2024. The Author(s).
Conflict of interest statement
J.C. is a shareholder and director of D-Gen, Ltd., an academic spin-out company working in the field of prion disease diagnosis, decontamination and therapeutics. D-Gen supplied the ICSM35 antibody used for PrP immunohistochemistry. The other authors declare no competing interests.
Figures

References
-
- Collinge J. Mammalian prions and their wider relevance in neurodegenerative diseases. Nature. 2016;539:217–226. - PubMed
-
- Collinge J, et al. Kuru in the 21st century—an acquired human prion disease with very long incubation periods. Lancet. 2006;367:2068–2074. - PubMed
-
- Mead S, et al. Balancing selection at the prion protein gene consistent with prehistoric kurulike epidemics. Science. 2003;300:640–643. - PubMed
-
- Collinge J, Sidle KC, Meads J, Ironside J, Hill AF. Molecular analysis of prion strain variation and the aetiology of ‘new variant’ CJD. Nature. 1996;383:685–690. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
