

Demographic and imaging features of oral squamous cell cancer in Serbia: a retrospective cross-sectional study
- PMID: 38287310
- PMCID: PMC10823646
- DOI: 10.1186/s12903-024-03869-8
Demographic and imaging features of oral squamous cell cancer in Serbia: a retrospective cross-sectional study
Abstract
Background: The mortality of oral squamous cell cancer (OSCC) in Serbia increased in the last decade. Recent studies on the Serbian population focused mainly on the epidemiological aspect of OSCC. This study aimed to investigate the demographic and imaging features of OSCC in the Serbian population at the time of diagnosis.
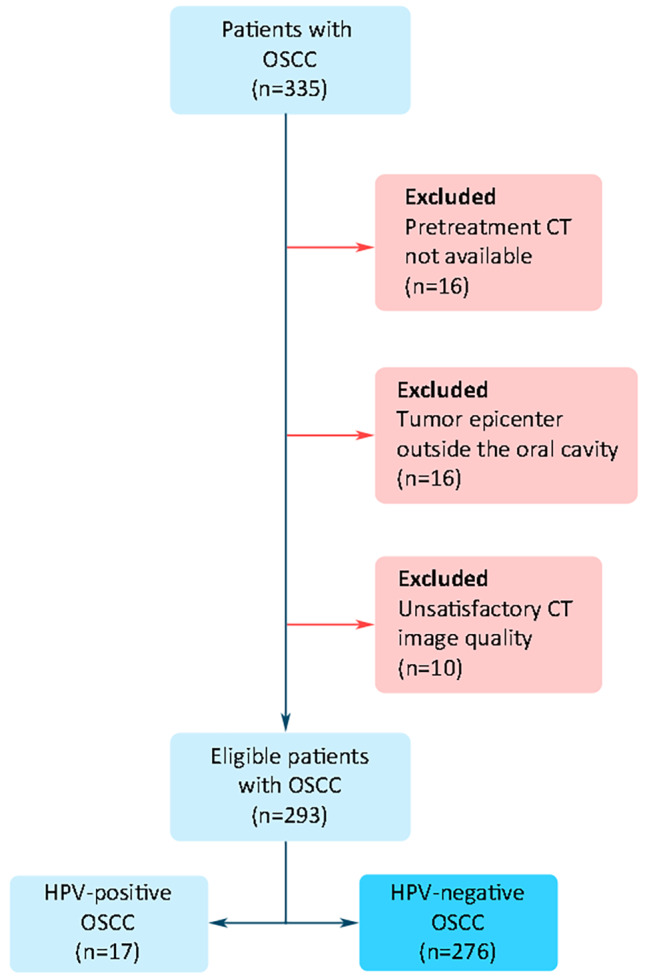
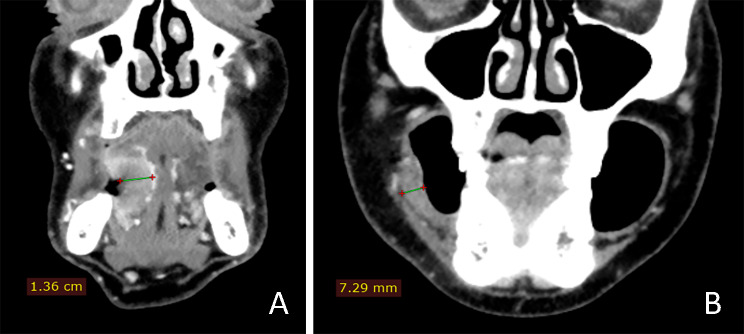
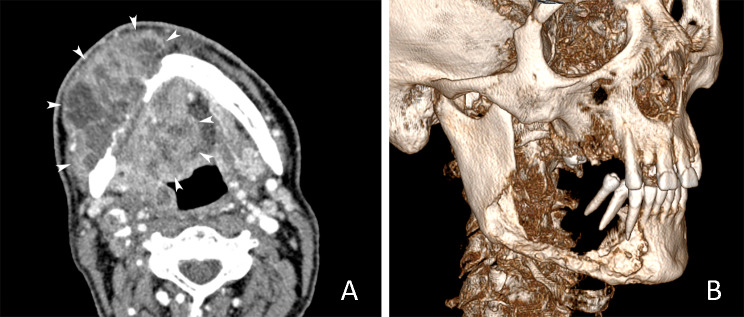
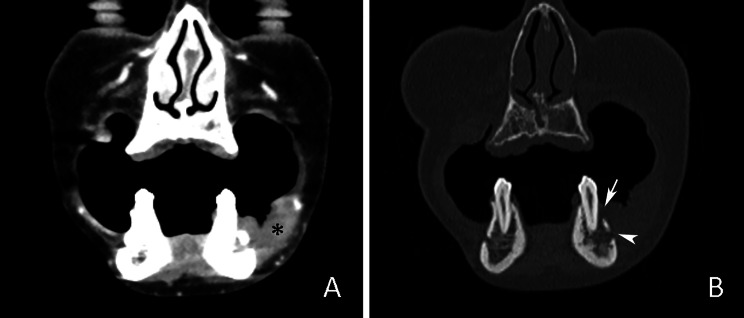
Methods: We retrospectively analyzed computed tomography (CT) images of 276 patients with OSCC diagnosed between 2017 and 2022. Age, gender, tumor site, tumor volume (CT-TV, in cm3), depth of invasion (CT-DOI, in mm), and bone invasion (CT-BI, in %) were evaluated. TNM status and tumor stage were also analyzed. All parameters were analyzed with appropriate statistical tests.
Results: The mean age was 62.32 ± 11.39 and 63.25 ± 11.71 for males and females, respectively. Male to female ratio was 1.63:1. The tongue (36.2%), mouth floor (21.0%), and alveolar ridge (19.9%) were the most frequent sites of OSCC. There was a significant gender-related difference in OSCC distribution between oral cavity subsites (Z=-4.225; p < 0.001). Mean values of CT-TV in males (13.8 ± 21.5) and females (5.4 ± 6.8) were significantly different (t = 4.620; p < 0.001). CT-DOI also differed significantly (t = 4.621; p < 0.001) between males (14.4 ± 7.4) and females (10.7 ± 4.4). CT-BI was detected in 30.1%, the most common in the alveolar ridge OSCC. T2 tumor status (31.4%) and stage IVA (28.3%) were the most dominant at the time of diagnosis. Metastatic lymph nodes were detected in 41.1%.
Conclusion: Our findings revealed significant gender-related differences in OSCC imaging features. The predominance of moderate and advanced tumor stages indicates a long time interval to the OSCC diagnosis.
Keywords: Demography; Oral cavity; Retrospective studies; Squamous cell Cancer; X-Ray computed Tomography.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Diz P, Meleti M, Diniz-Freitas M, Vescovi P, Warnakulasuriya S, Johnson NW et al. Oral and pharyngeal cancer in Europe: incidence, mortality and trends as presented to the global oral Cancer Forum. Transl Res Oral Oncol. 2017;2.
-
- Abed H, Reilly D, Burke M, Daly B. Patients with head and neck cancers’ oral health knowledge, oral health-related quality of life, oral health status, and adherence to advice on discharge to primary dental care: a prospective observational study. Spec Care Dentist. 2019;39:593–602. doi: 10.1111/scd.12418. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
