

Is the price right? Paying for value today to get more value tomorrow
- PMID: 38287326
- PMCID: PMC10826180
- DOI: 10.1186/s12916-024-03262-w
Is the price right? Paying for value today to get more value tomorrow
Abstract
Background: Contemporary debates about drug pricing feature several widely held misconceptions, including the relationship between incentives and innovation, the proportion of total healthcare spending on pharmaceuticals, and whether the economic evaluation of a medicine can be influenced by things other than clinical efficacy.
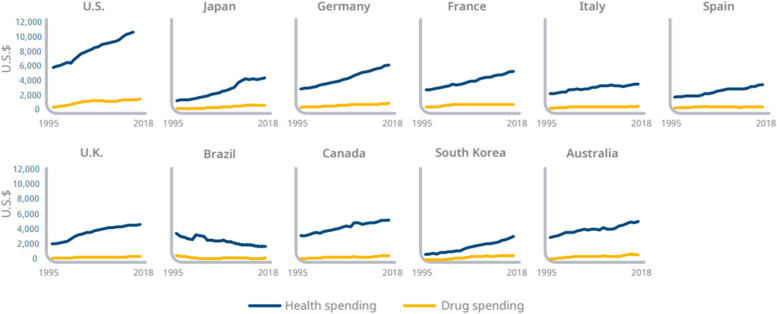
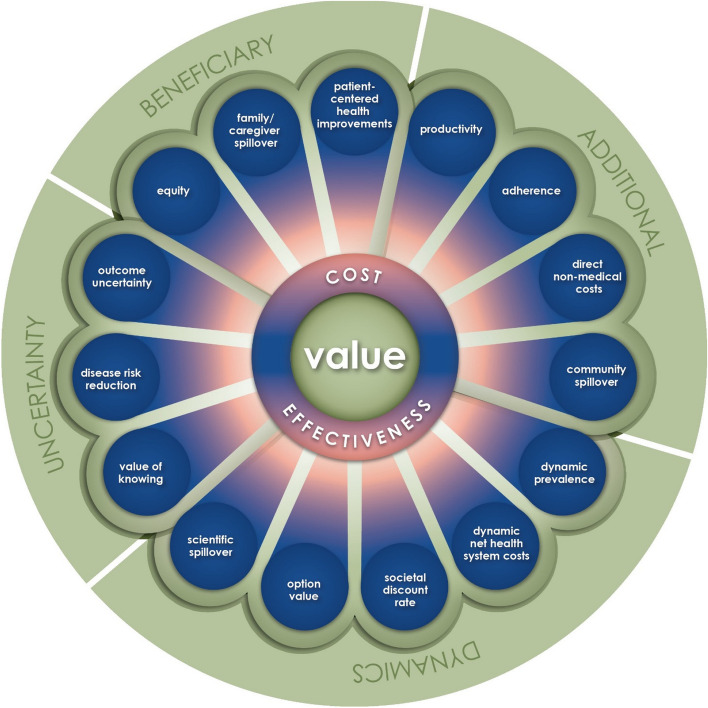
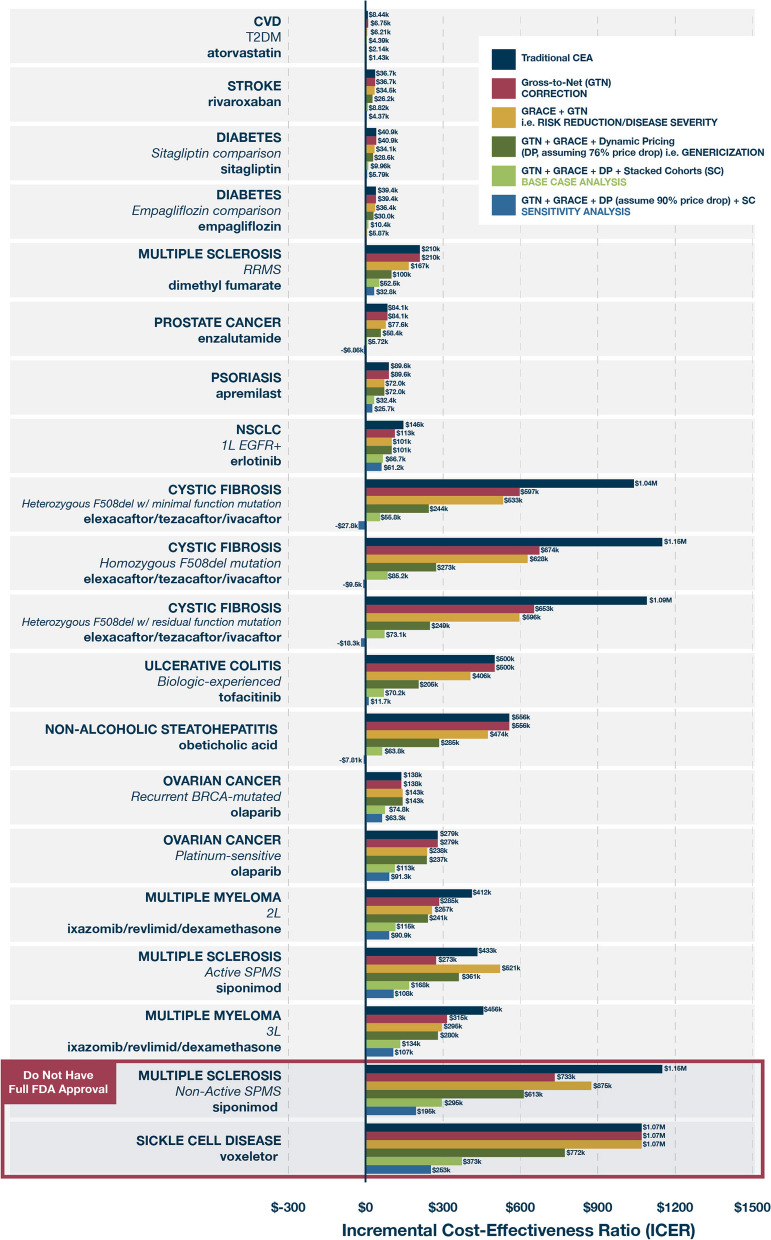
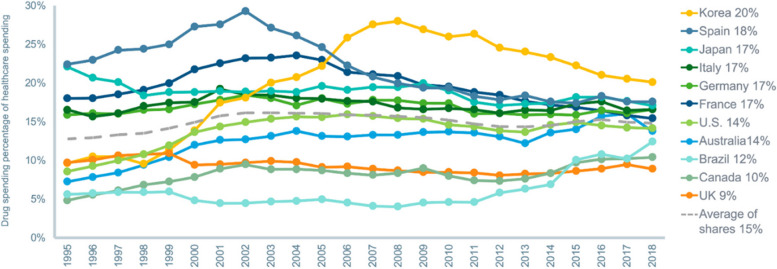
Main body: All citizens should have access to timely, equitable, and cost-effective care covered by public funds, private insurance, or a combination of both. Better managing the collective burden of diseases borne by today's and future generations depends in part on developing better technologies, including better medicines. As in any innovative industry, the expectation of adequate financial returns incentivizes innovators and their investors to develop new medicines. Estimating expected returns requires that they forecast revenues, based on the future price trajectory and volume of use over time. How market participants decide what price to set or accept can be complicated, and some observers and stakeholders want to confirm whether the net prices society pays for novel medicines, whether as a reward for past innovation or an incentive for future innovation, are commensurate with those medicines' incremental value. But we must also ask "value to whom?"; medicines not only bring immediate clinical benefits to patients treated today, but also can provide a broad spectrum of short- and long-term benefits to patients, their families, and society. Spending across all facets of healthcare has grown over the last 25 years, but both inpatient and outpatient spending has outpaced drug spending growth even as our drug armamentarium is constantly improving with safer and more effective medicines. In large part, this is because, unlike hospitals, drugs typically go generic, thus making room in our budgets for new and better ones, even as they often keep patients out of hospitals, driving further savings.
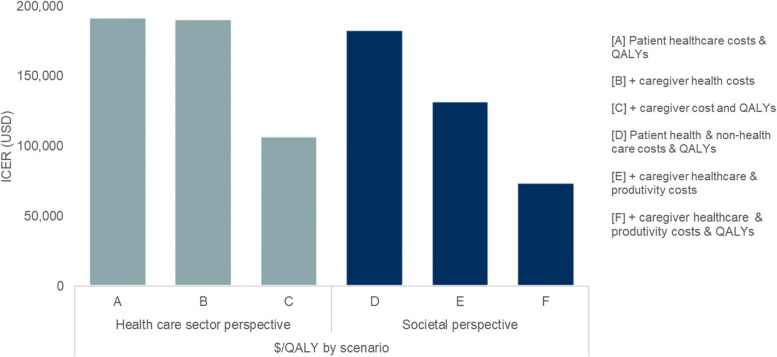
Conclusion: A thorough evaluation of drug spending and value can help to promote a better allocation of healthcare resources for both the healthy and the sick, both of whom must pay for healthcare. Taking a holistic approach to assessing drug value makes it clear that a branded drug's value to a patient is often only a small fraction of the drug's total value to society. Societal value merits consideration when determining whether and how to make a medicine affordable and accessible to patients: a drug that is worth its price to society should not be rendered inaccessible to ill patients by imposing high out-of-pocket costs or restricting coverage based on narrow health technology assessments (HTAs). Furthermore, recognizing the total societal cost of un- or undertreated conditions is crucial to gaining a thorough understanding of what guides the biomedical innovation ecosystem to create value for society. It would be unwise to discourage the development of new solutions without first appreciating the cost of leaving the problems unsolved.
Keywords: Cost-effectiveness; Drug; Health technology assessment; Inflation reduction act; Medicine; Pricing; Value.
© 2024. The Author(s).
Conflict of interest statement
SR and GM are employees of Lane Clark and Peacock. JD is an employee and shareholder of Bristol Myers Squibb. LG has consulted for a number of pharmaceutical companies. PK is the Managing Director of RA Capital.
Figures
References
-
- Ramagopalan S, Leahy TP, Ray J, Wilkinson S, Sammon C, Subbiah V. The value of innovation: association between improvements in survival of advanced and metastatic non-small cell lung cancer and targeted and immunotherapy. BMC Med. 2021;19(1):209. doi: 10.1186/s12916-021-02070-w. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
