

Human Trypanosoma cruzi infection in the Argentinean Chaco: risk factors and identification of households with infected children for treatment
- PMID: 38287434
- PMCID: PMC10826042
- DOI: 10.1186/s13071-024-06125-8
Human Trypanosoma cruzi infection in the Argentinean Chaco: risk factors and identification of households with infected children for treatment
Abstract
Background: Chagas disease is a neglected tropical disease (NTD). Cost-effective strategies for large-scale implementation of diagnosis and etiological treatment are urgently needed to comply with NTD control goals. We determined the seroprevalence of Trypanosoma cruzi infection and associated risk factors in a well-defined rural population of Pampa del Indio municipality including creole and indigenous (Qom) households and developed two indices to identify houses harboring infected children.
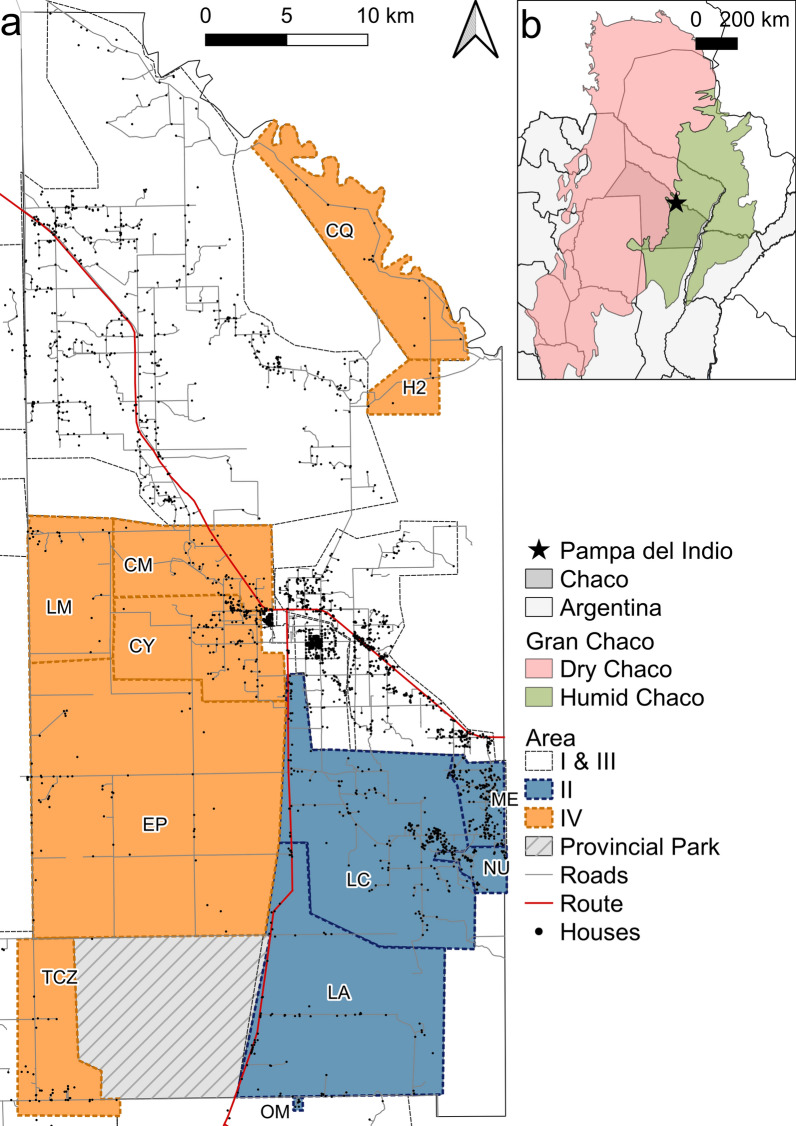
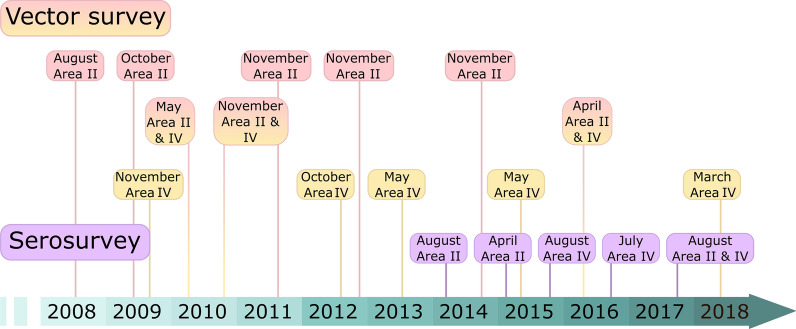
Methods: We serodiagnosed and administered a questionnaire to 1337 residents (48.2% of the listed population) in two sections of the municipality (named Areas II and IV) 6-9 years after deploying sustained vector control interventions. Multiple logistic regression models were used to evaluate the relationship between human infection and a priori selected predictors. Two risk indices were constructed based on environmental and serostatus variables, and we used spatial analysis to test whether households harboring T. cruzi-seropositive children were randomly distributed.
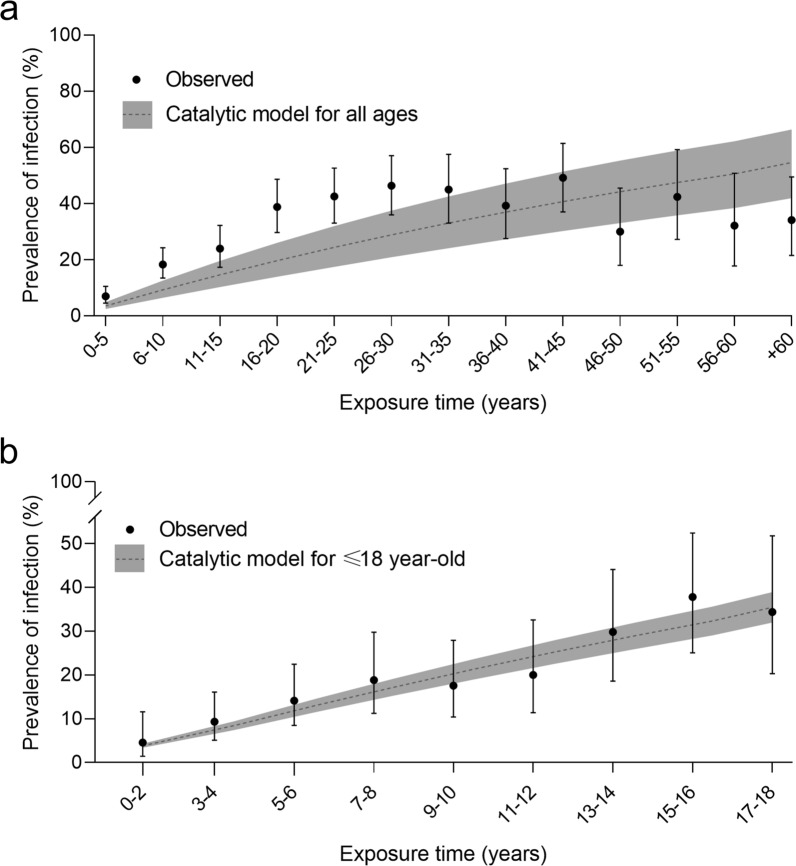
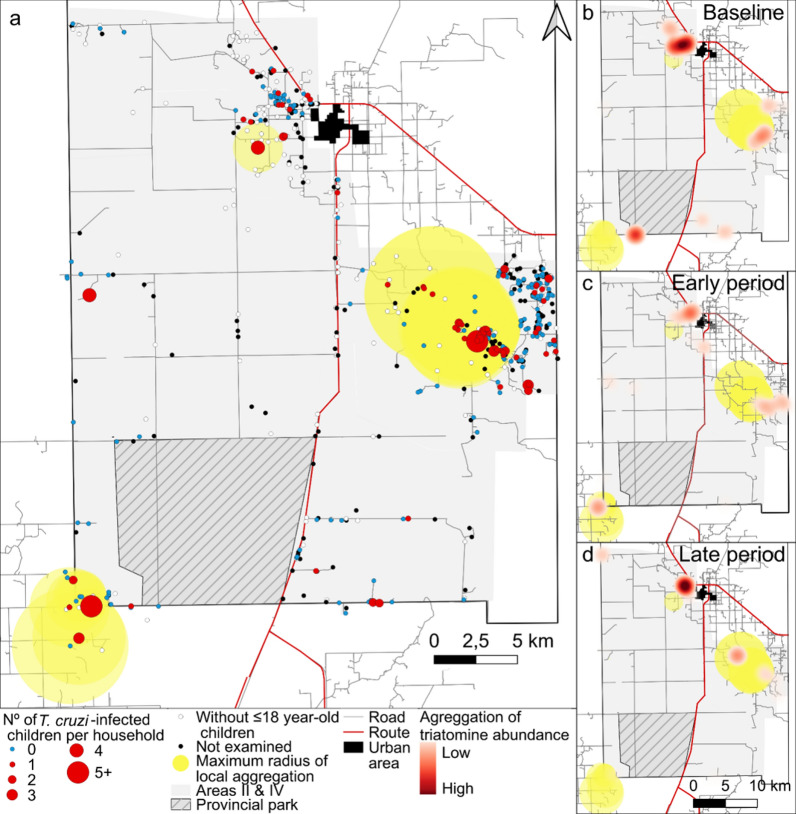
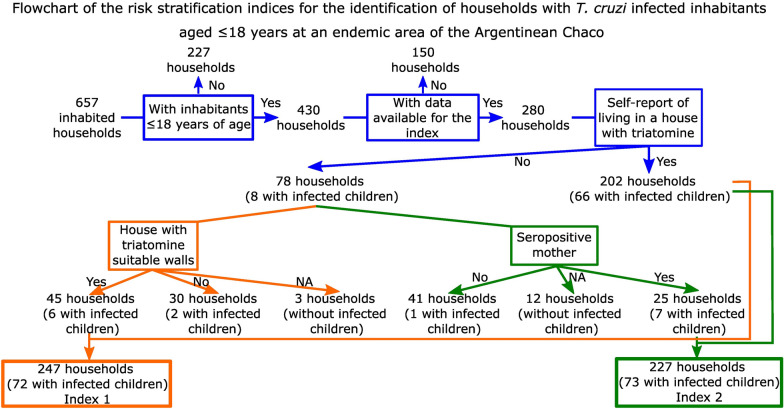
Results: The global seroprevalence of T. cruzi infection was 24.8%. Human infection was positively and significantly associated with exposure time to triatomines, the household number of seropositive co-inhabitants, maternal seropositivity for T. cruzi, recent residence at the current house and the presence of suitable walls for triatomine colonization in the domicile. The pre-intervention mean annual force of infection (FOI) was 1.23 per 100 person-years. Creoles from Area IV exhibited the highest seroprevalence and FOI; Qom people from both areas displayed intermediate ones and creoles from Area II the lowest. Three hotspots of infected children were spatially associated with hotspots of triatomine abundance at baseline and persistent house infestation. No child born after vector control interventions was T. cruzi seropositive except for one putative transplacental case. Two simple risk indices (based on self-reported inhabiting an infested house and suitable walls for triatomines or maternal serostatus) identified 97.3-98.6% of the households with at least one T. cruzi-seropositive child.
Conclusions: We showed strong heterogeneity in the seroprevalence of T. cruzi infection within and between ethnic groups inhabiting neighboring rural areas. Developed indices can be used for household risk stratification and to improve access of rural residents to serodiagnosis and treatment and may be easily transferred to primary healthcare personnel.
Keywords: Chagas disease; Indigenous; Risk factor; Seroprevalence; Stratification; Trypanosoma cruzi.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Hotez PJ, Bottazzi ME, Franco-Paredes C, Ault SK, Periago MR. The neglected tropical diseases of Latin America and the Caribbean: a review of disease burden and distribution and a roadmap for control and elimination. PLoS Negl Trop Dis. 2008;2:e300. doi: 10.1371/journal.pntd.0000300. - DOI - PMC - PubMed
-
- Ault SK. Chagas Disease and neglected diseases: changing poverty and exclusion. Am Ancestral: Organización Panamericana de la Salud; 2007. pp. 13–18.
-
- WHO . Ending the neglect to attain the sustainable development goals: a road map for neglected tropical diseases 2021–2030. Geneva: World Health Organization; 2020.
-
- World Health Organization . Control of Chagas Disease : second report of the WHO expert committee. Geneva: WHO; 2002. pp. 1–109. - PubMed
MeSH terms
Supplementary concepts
Grants and funding
- UBACYT 20020100100944 and 20020130100843BA/Universidad de Buenos Aires
- UBACYT 20020100100944 and 20020130100843BA/Universidad de Buenos Aires
- UBACYT 20020100100944 and 20020130100843BA/Universidad de Buenos Aires
- UBACYT 20020100100944 and 20020130100843BA/Universidad de Buenos Aires
- UBACYT 20020100100944 and 20020130100843BA/Universidad de Buenos Aires
- UBACYT 20020100100944 and 20020130100843BA/Universidad de Buenos Aires
- PICT 2014-2661, PICT 2015-2921/Agencia Nacional de Promoción Científica y Tecnológica
- PICT 2014-2661, PICT 2015-2921/Agencia Nacional de Promoción Científica y Tecnológica
- PICT 2014-2661, PICT 2015-2921/Agencia Nacional de Promoción Científica y Tecnológica
- PICT 2014-2661, PICT 2015-2921/Agencia Nacional de Promoción Científica y Tecnológica
- PICT 2014-2661, PICT 2015-2921/Agencia Nacional de Promoción Científica y Tecnológica
- PICT 2014-2661, PICT 2015-2921/Agencia Nacional de Promoción Científica y Tecnológica
- Avia Terai sin Chagas/Fundación Bunge y Born
- Avia Terai sin Chagas/Fundación Bunge y Born
- Avia Terai sin Chagas/Fundación Bunge y Born
- Avia Terai sin Chagas/Fundación Bunge y Born
- Avia Terai sin Chagas/Fundación Bunge y Born
- Avia Terai sin Chagas/Fundación Bunge y Born
LinkOut - more resources
Full Text Sources
Medical
