

Hospital outpatient department billing is a poor indicator of primary care practice integration with hospital systems
- PMID: 38287519
- PMCID: PMC10915492
- DOI: 10.1111/1475-6773.14284
Hospital outpatient department billing is a poor indicator of primary care practice integration with hospital systems
Abstract
Objective: To test the reliability of Medicare claims in measuring vertical integration. We assess the accuracy of a commonly used measure of integration, primary care physician (PCP) practices billing Medicare as a hospital outpatient department (HOPD) in claims.
Data sources and study setting: Medicare fee-for-service claims, IQVIA, and CPC+ practice surveys for this study.
Study design: We compare measures of integration from Medicare claims to self-reported indicators of integration from IQVIA and a survey of CPC+ participating practice sites.
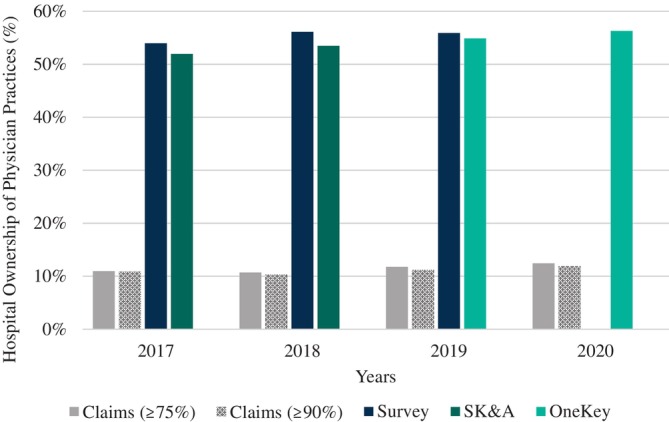
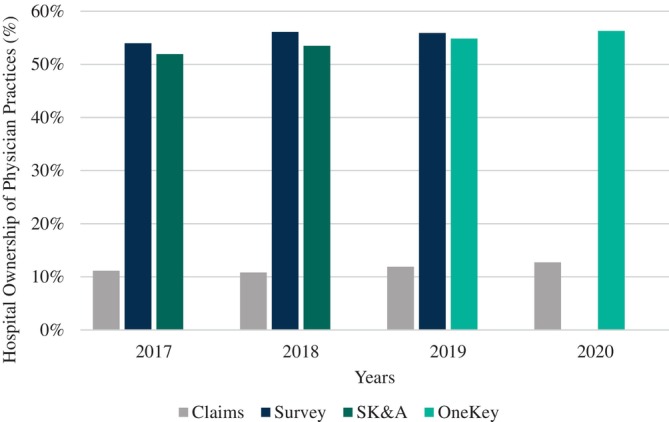
Data collection/extraction methods: We measure integration by using site-of-service billing in the 100% sample of Medicare Carrier claims from 2017-2020. In the IQVIA SK&A (2017-2018), OneKey (2019-2020), and practice survey data (2017-2019), we use self-reported responses to measure integration.
Principal findings: We find that currently most PCP practices sites that report themselves as being integrated with a health system do not bill as an HOPD. In 2017, 11% of CPC+ practices were identified as being vertically integrated in claims, while the equivalent numbers in SK&A and surveys were 52% and 54% integration, respectively. A t-test found that both datasets significantly differed from claims (Survey: 41.3%-45.1%; SK&A: 45.3%-51.1%); this gap persists in 2018-2019.
Conclusion: Measuring physician-hospital vertical integration accurately is integral to determining consolidation. The overwhelming majority of PCP practice sites not billing as an HOPD may reflect Medicare regulatory changes that have reduced the financial incentives for doing so. These findings have implications for researchers that study the growth in PCP-hospital integration in health care markets.
Keywords: health care organizations and systems; hospitals; ownership/governance.
© 2024 Health Research and Educational Trust.
Figures
References
-
- O'Malley AS, Bond AM, Berenson RA. Rising hospital employment of physicians: better quality costs. Center for Studying Health Systems Change? 2011;(136):5. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
