

Preeclampsia-Associated Cardiovascular Risk Factors 6 Months and 2 Years After Pregnancy: The P4 Study
- PMID: 38288610
- PMCID: PMC10956664
- DOI: 10.1161/HYPERTENSIONAHA.123.21890
Preeclampsia-Associated Cardiovascular Risk Factors 6 Months and 2 Years After Pregnancy: The P4 Study
Abstract
Background: Increased cardiovascular risk following preeclampsia is well established and there are signs of early cardiovascular aging 6 months postpartum. This study assessed whether blood pressure (BP) and other cardiovascular measures are abnormal 2 years postpartum in the same cohort to determine ongoing risk markers.
Methods: Six months and 2 years postpartum, BP was measured using sphygmomanometry, 24-hour ambulatory BP monitoring, and noninvasive central BP. Anthropometric measures, blood, and urine biochemistry were performed. Cross-sectional comparisons between preeclampsia and normotensive pregnancy (NP) groups and longitudinal comparisons within each group were made at 6 months and 2 years.
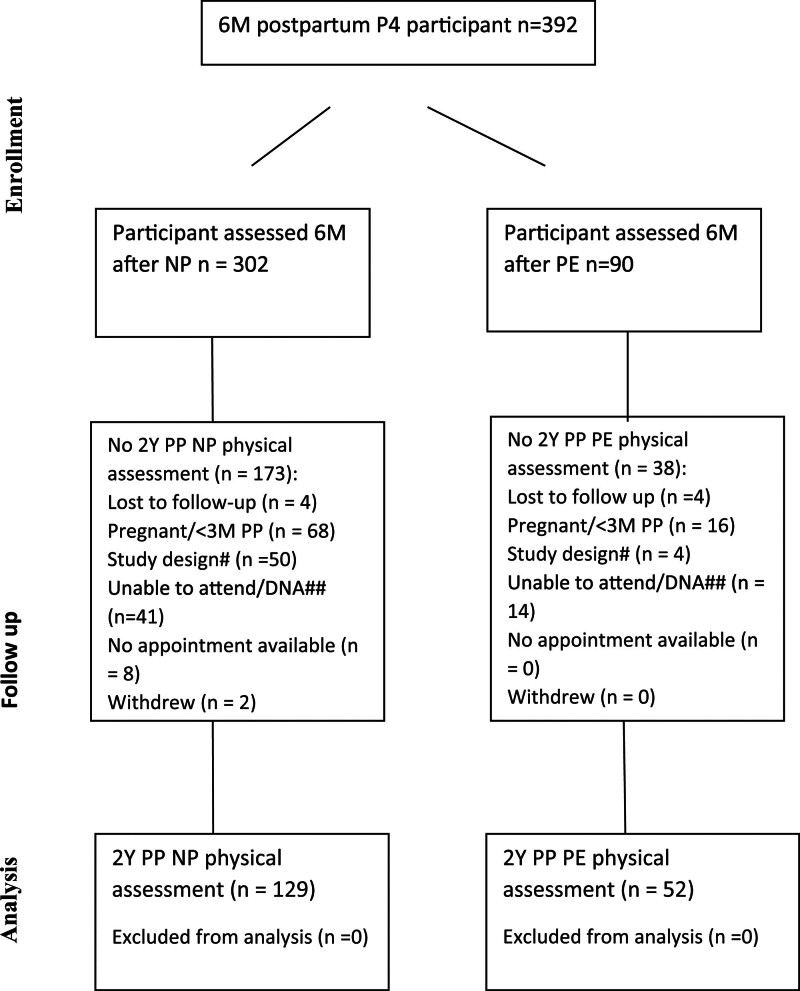
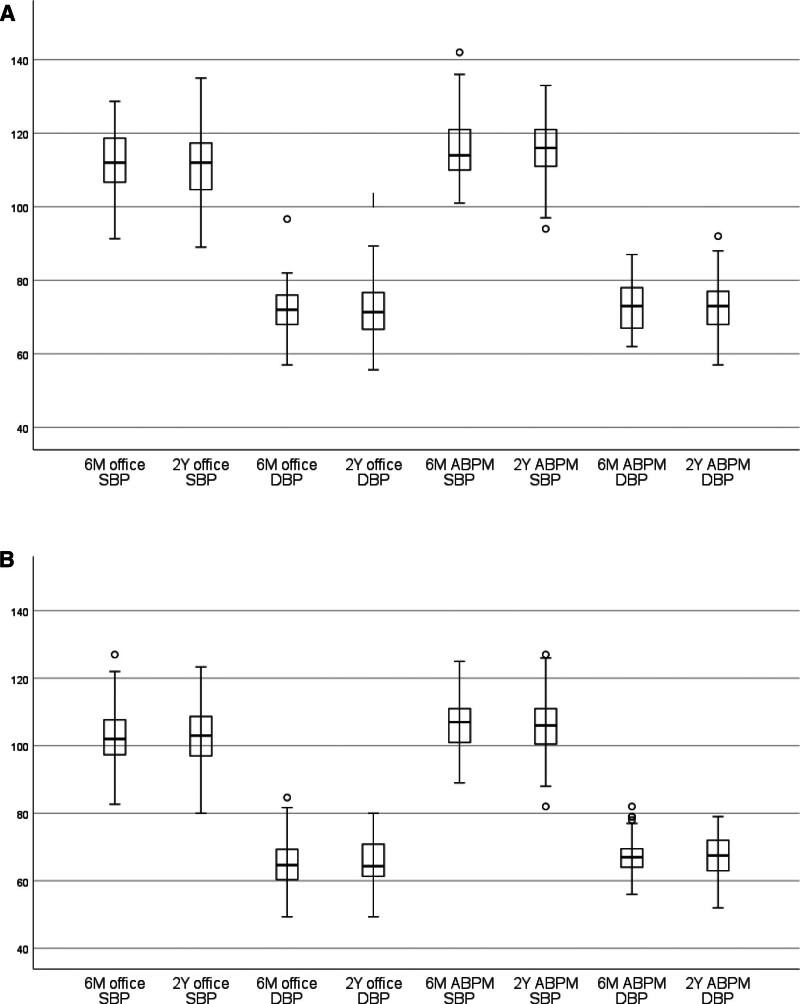
Results: Two years postpartum, 129 NP, and 52 preeclampsia women were studied who also had 6 months measures. At both time points, preeclampsia group had significantly higher BP (office BP 2 years, 112±12/72±8 versus 104±9/67±7 mm Hg NP; [P<0.001]; mean ambulatory BP monitoring 116±9/73±8 versus 106±8/67±6 mm Hg NP; [P<0.001]). No significant BP changes noted 6 months to 2 years within either group. Office BP thresholds of 140 mm Hg systolic and 90 mm Hg diastolic classified 2% preeclampsia and 0% NP at 2 years. American Heart Association 2017 criteria (above normal, >120/80 mm Hg) classified 25% versus 8% (P<0.002), as did our reference range threshold of 122/79 mm Hg. American Heart Association criteria classified 60% post-preeclampsia versus 16% after NP with above-normal ambulatory BP monitoring (P<0.001). Other cardiovascular risk markers more common 2 years post-preeclampsia included higher body mass index (median 26.6 versus 23.1, P=0.003) and insulin resistance.
Conclusions: After preeclampsia, women have significantly higher BP 6 months and 2 years postpartum, and have higher body mass index and insulin-resistance scores, increasing their future cardiovascular risk. Regular cardiovascular risk screening should be implemented for all who have experienced preeclampsia.
Keywords: cardiovascular diseases; hypertension; longitudinal studies; postpartum period; pre-eclampsia; risk factors.
Conflict of interest statement
None.
Figures
Similar articles
-
Recognizing Cardiovascular Risk After Preeclampsia: The P4 Study.J Am Heart Assoc. 2020 Nov 17;9(22):e018604. doi: 10.1161/JAHA.120.018604. Epub 2020 Nov 10. J Am Heart Assoc. 2020. PMID: 33170079 Free PMC article.
-
The P4 study: Subsequent pregnancy maternal physiology after hypertensive and normotensive pregnancies.Pregnancy Hypertens. 2022 Mar;27:29-34. doi: 10.1016/j.preghy.2021.10.004. Epub 2021 Oct 30. Pregnancy Hypertens. 2022. PMID: 34864294
-
Prevalence of Hypertensive Phenotypes After Preeclampsia: A Prospective Cohort Study.Hypertension. 2018 Jan;71(1):103-109. doi: 10.1161/HYPERTENSIONAHA.117.09799. Epub 2017 Nov 13. Hypertension. 2018. PMID: 29133363
-
Risk of future cardiovascular diseases in different years postpartum after hypertensive disorders of pregnancy: A systematic review and meta-analysis.Medicine (Baltimore). 2022 Jul 29;101(30):e29646. doi: 10.1097/MD.0000000000029646. Medicine (Baltimore). 2022. PMID: 35905265 Free PMC article.
-
Preeclampsia Emerging as a Risk Factor of Cardiovascular Disease in Women.High Blood Press Cardiovasc Prev. 2021 Mar;28(2):103-114. doi: 10.1007/s40292-020-00425-7. Epub 2021 Mar 3. High Blood Press Cardiovasc Prev. 2021. PMID: 33660234 Review.
Cited by
-
Gender Differences in Blood Pressure Control Among Hypertensive Patients: A Cross-Sectional Study at a Tertiary Hospital.J Clin Hypertens (Greenwich). 2025 Jan;27(1):e14975. doi: 10.1111/jch.14975. J Clin Hypertens (Greenwich). 2025. PMID: 39823136 Free PMC article.
-
Role of biomarkers in identifying women at risk of hypertension and renal dysfunction on follow-up after severe preeclampsia.J Hum Hypertens. 2025 Aug;39(8):572-579. doi: 10.1038/s41371-024-00981-8. Epub 2025 Jul 10. J Hum Hypertens. 2025. PMID: 40640616
-
Analysis of serological risk factors for preeclampsia and the predictive role of high homocysteine levels.Am J Transl Res. 2025 May 15;17(5):3465-3475. doi: 10.62347/IKIP3300. eCollection 2025. Am J Transl Res. 2025. PMID: 40535685 Free PMC article.
-
Advances in Our Understanding of Cardiovascular Diseases After Preeclampsia.Circ Res. 2025 Mar 14;136(6):583-593. doi: 10.1161/CIRCRESAHA.124.325581. Epub 2025 Mar 13. Circ Res. 2025. PMID: 40080539 Review.
-
Metabolic outcomes in women 6 months and 2 years after preeclampsia versus normotensive pregnancy: A P4 study.Clin Obes. 2025 Feb;15(1):e12706. doi: 10.1111/cob.12706. Epub 2024 Oct 8. Clin Obes. 2025. PMID: 39377496 Free PMC article.
References
-
- Magee L, Brown M, Hall D, Gupte S, Hennessy A, Karumanchi S, Kenny L, McCarthy F, Myers J, Poon L, et al. . The hypertensive disorders of pregnancy: the 2021 International Society for the Study of Hypertension in Pregnancy Classification, Diagnosis & Management Recommendations for International Practice. Pregnancy Hypertens. 2022;27:148–169. doi: 10.1016/j.preghy.2021.09.008 - PubMed
-
- Wu P, Haththotuwa R, Kwok C, Babu A, Kotronias R, Rushton C, Zaman A, Fryer A, Kadam U, Chew-Graham C, et al. . Preeclampsia and future cardiovascular health: a systematic review and meta-analysis. Circ Cardiovasc Qual Outcomes. 2017;10:e003497. doi: 10.1161/CIRCOUTCOMES.116.003497 - PubMed
-
- Leon L, McCarthy F, Direk K, Gonzalez-Izquierdo A, Prieto-Merino D, Casas J, Chappell L. Preeclampsia and cardiovascular disease in a large UK pregnancy cohort of linked electronic health records: a CALIBER study. Circulation. 2019;140:1050–1060. doi: 10.1161/CIRCULATIONAHA.118.038080 - PubMed
-
- Arnott C, Nelson M, Alfaro Ramirez M, Hyett J, Gale M, Henry A, Celermajer D, Taylor L, Woodward M. Maternal cardiovascular risk after hypertensive disorder of pregnancy. Heart. 2020;106:1927–1933. doi: 10.1136/heartjnl-2020-316541 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
