

Ebstein's anomaly: an electrophysiological perspective
- PMID: 38289561
- PMCID: PMC11166840
- DOI: 10.1007/s10840-024-01744-8
Ebstein's anomaly: an electrophysiological perspective
Abstract
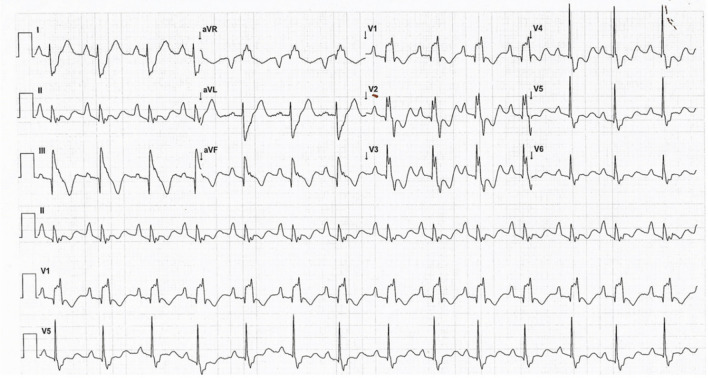
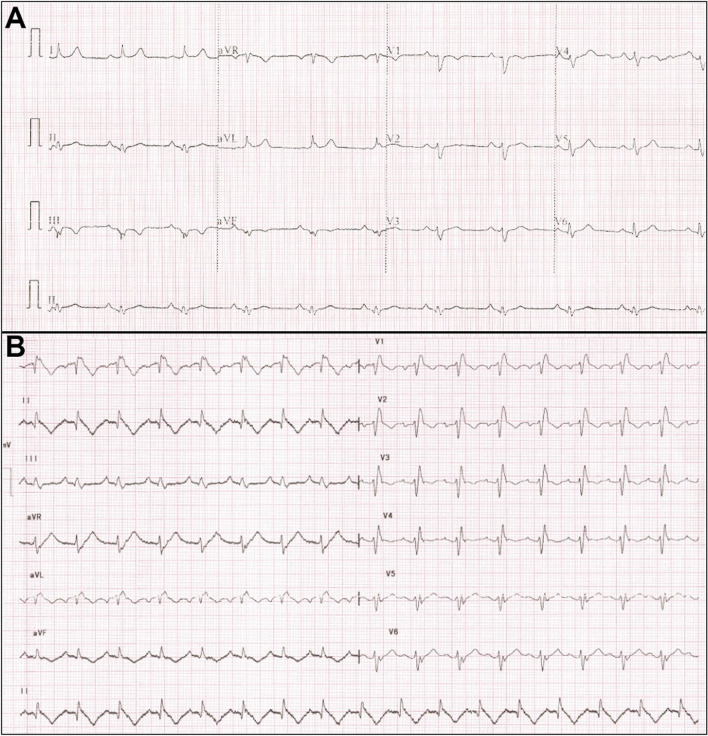
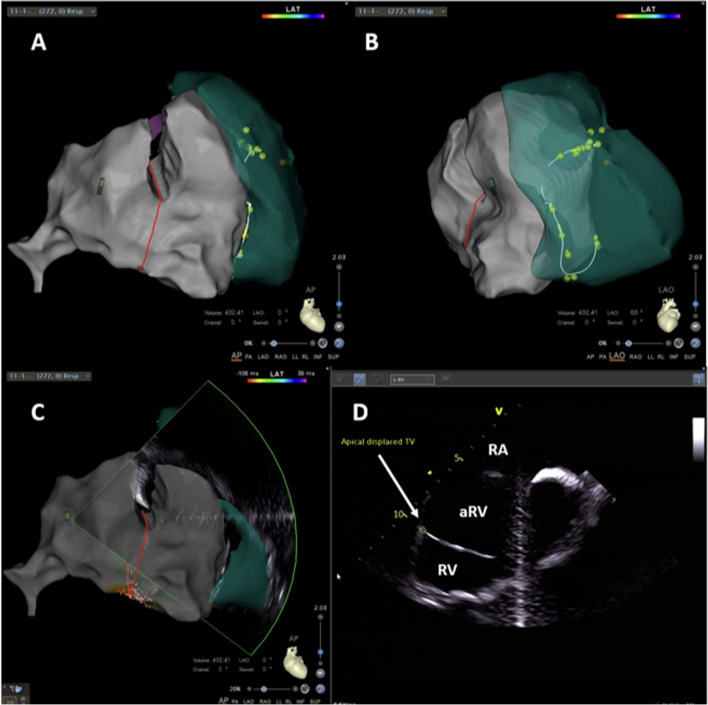
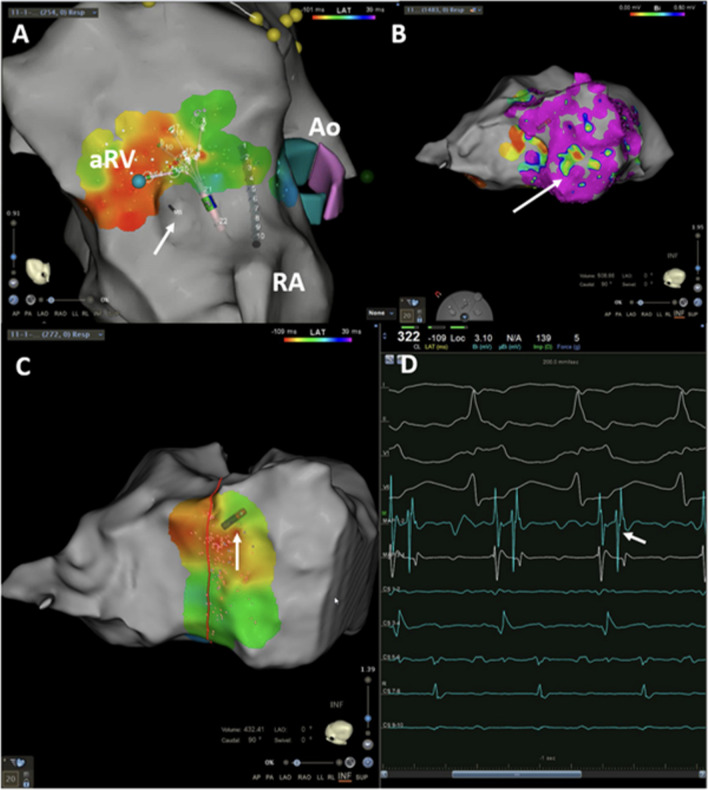
Ebstein's anomaly of the tricuspid valve (EA) is an uncommon congenital cardiac malformation. It can present with atrioventricular tachycardia (AVRT), atrioventricular nodal re-entrant tachycardia (AVNRT), atrial arrhythmias, and rarely with ventricular tachycardia. The 12-lead electrocardiogram (ECG) is critically important and often diagnostic even prior to an electrophysiology study (EPS). Due to its complex anatomy, it poses particular challenges for mapping and ablation, even for an experienced electrophysiologist. In this review, we aim to provide insight into the electrophysiological perspective of EA and an in-depth analysis of the various arrhythmias encountered in diverse clinical scenarios.
Keywords: Ablation; Arrhythmia; Ebstein anomaly.
© 2024. Crown.
Conflict of interest statement
Dr Saurabh Kumar is supported by the NSW Health Early Mid-Career Fellowship. Timothy Campbell has received speakers’ honoraria for Biosense Webster. All other authors declare no competing interests.
Figures


References
-
- Becker AE, Becker MJ, Edwards JE. Pathologic spectrum of dysplasia of the tricuspid valve. Features in common with Ebstein’s malformation. Arch Pathol. 1971;91(2):167–78. - PubMed
-
- Lev M, Liberthson RR, Joseph RH, Seten CE, Eckner FA, Kunske RD, et al. The pathologic anatomy of Ebstein’s disease. Arch Pathol. 1970;90(4):334–343. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
