

Electrical storm treatment by percutaneous stellate ganglion block: the STAR study
- PMID: 38289867
- PMCID: PMC10919918
- DOI: 10.1093/eurheartj/ehae021
Electrical storm treatment by percutaneous stellate ganglion block: the STAR study
Erratum in
-
Correction to: Electrical storm treatment by percutaneous stellate ganglion block: the STAR study.Eur Heart J. 2024 Oct 14;45(39):4235. doi: 10.1093/eurheartj/ehae631. Eur Heart J. 2024. PMID: 39287435 Free PMC article. No abstract available.
Abstract
Background and aims: An electrical storm (ES) is a clinical emergency with a paucity of established treatment options. Despite initial encouraging reports about the safety and effectiveness of percutaneous stellate ganglion block (PSGB), many questions remained unsettled and evidence from a prospective multicentre study was still lacking. For these purposes, the STAR study was designed.
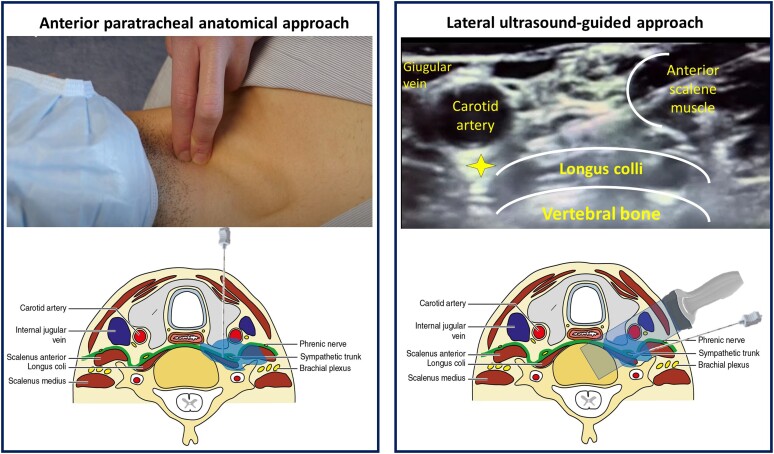
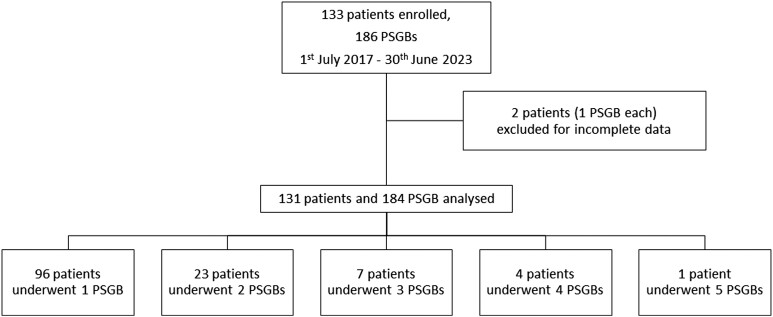
Methods: This is a multicentre observational study enrolling patients suffering from an ES refractory to standard treatment from 1 July 2017 to 30 June 2023. The primary outcome was the reduction of treated arrhythmic events by at least 50% comparing the 12 h following PSGB with the 12 h before the procedure. STAR operators were specifically trained to both the anterior anatomical and the lateral ultrasound-guided approach.
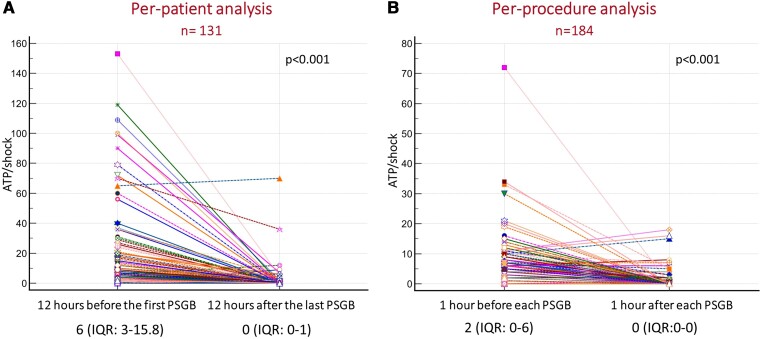
Results: A total of 131 patients from 19 centres were enrolled and underwent 184 PSGBs. Patients were mainly male (83.2%) with a median age of 68 (63.8-69.2) years and a depressed left ventricular ejection fraction (25.0 ± 12.3%). The primary outcome was reached in 92% of patients, and the median reduction of arrhythmic episodes between 12 h before and after PSGB was 100% (interquartile range -100% to -92.3%). Arrhythmic episodes requiring treatment were significantly reduced comparing 12 h before the first PSGB with 12 h after the last procedure [six (3-15.8) vs. 0 (0-1), P < .0001] and comparing 1 h before with 1 h after each procedure [2 (0-6) vs. 0 (0-0), P < .001]. One major complication occurred (0.5%).
Conclusions: The findings of this large, prospective, multicentre study provide evidence in favour of the effectiveness and safety of PSGB for the treatment of refractory ES.
Keywords: Electrical storm; Neuromodulation; Stellate ganglion block; Ventricular tachycardia.
© The Author(s) 2024. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures


References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
